Ross & Wilson Anatomy and Physiology in Health and Illness (209 page)
Read Ross & Wilson Anatomy and Physiology in Health and Illness Online
Authors: Anne Waugh,Allison Grant
Tags: #Medical, #Nursing, #General, #Anatomy

The penis (
Fig. 18.17
) has a
root
and a
body
. The root lies in the perineum and the body surrounds the urethra. It is formed by three cylindrical masses of
erectile tissue
and smooth muscle. The erectile tissue is supported by fibrous tissue and covered with skin and has a rich blood supply.
The two lateral columns are called the
corpora cavernosa
and the column between them, containing the urethra, is the
corpus spongiosum
. At its tip it is expanded into a triangular structure known as the
glans penis
. Just above the glans the skin is folded upon itself and forms a movable double layer, the
foreskin
or
prepuce
. Arterial blood is supplied by deep, dorsal and bulbar arteries of the penis, which are branches from the internal pudendal arteries. A series of veins drain blood to the internal pudendal and internal iliac veins. The penis is supplied by autonomic and somatic nerves. Parasympathetic stimulation leads to filling of the spongy erectile tissue with blood, caused by arteriolar dilation and venoconstriction, which increases blood flow into the penis and obstructs outflow. The penis therefore becomes engorged and erect, essential for sexual intercourse.
Ejaculation
During ejaculation, which occurs at male orgasm, spermatozoa are expelled from the epididymis and pass through the deferent duct, the ejaculatory duct and the urethra. The semen is propelled by powerful rhythmical contraction of the smooth muscle in the walls of the deferent duct; the muscular contractions are sympathetically mediated. Muscle in the walls of the seminal vesicles and prostate gland also contracts, adding their contents to the fluid passing through the genital ducts. The force generated by these combined processes leads to emission of the semen through the external urethral sphincter (
Fig. 18.18
).
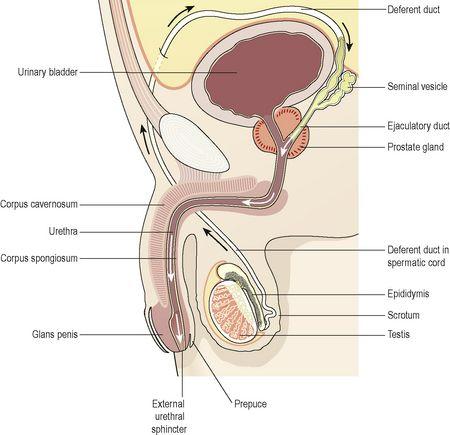
Figure 18.18
Section of the male reproductive organs.
Arrows show the route taken by spermatozoa during ejaculation.
Sperm comprise only 10% of the final ejaculate, the remainder being made up of seminal and prostatic fluids, which are added to the sperm during male orgasm, as well as mucus produced in the urethra. Semen is slightly alkaline, to neutralise the acidity of the vagina. Between 2 and 5 ml of semen are produced in a normal ejaculate, and contain between 40 and 100 million spermatozoa per ml. If not ejaculated, sperm gradually lose their fertility after several months and are reabsorbed by the epididymis.
Puberty in the male
This occurs between the ages of 10 and 14. Luteinising hormone from the anterior lobe of the pituitary gland stimulates the interstitial cells of the testes to increase the production of testosterone. This hormone influences the development of the body to sexual maturity. The changes occurring at puberty include:
•
growth of muscle and bone and a marked increase in height and weight
•
enlargement of the larynx and deepening of the voice – it ‘breaks’
•
growth of hair on the face, axillae, chest, abdomen and pubis
•
enlargement of the penis, scrotum and prostate gland
•
maturation of the seminiferous tubules and production of spermatozoa
•
the skin thickens and becomes oilier.
In the male, fertility and sexual ability tend to decline gradually with ageing. The secretion of testosterone gradually declines, usually beginning at about 50 years of age. There is no period comparable to the female menopause.
Sexually transmitted infections

Learning outcomes
After studying this section, you should be able to:
list the principal causes of sexually transmitted infections
This is common in all cultures and an increasing problem in many countries.
Micro-organisms responsible for sexually transmitted infections are unable to survive outside the body for long periods and have no intermediate host.
Chlamydia
The organism
Chlamydia trachomatis
causes inflammation of the female cervix. Infection may ascend through the reproductive tract and cause pelvic inflammatory disease (
p. 453
). In the male, it may cause urethritis, which may also ascend and lead to epididymitis. Chlamydia infection is often present in conjunction with other sexually transmitted diseases. The same organism causes trachoma, an eye infection that is the primary cause of blindness worldwide (
p. 205
).
Gonorrhoea
This is caused by
Neisseria gonorrhoeae
, which infects the mucosa of the reproductive and urinary tracts. In the male, suppurative urethritis occurs and the infection may spread to the prostate gland, epididymis and testes. In the female the infection may spread from vulvar glands, vagina and cervix to the body of the uterus, uterine tubes, ovaries and peritoneum. Healing by fibrosis in the female may cause obstruction of the uterine tubes, leading to infertility. In the male it may cause urethral stricture.
Non-venereal transmission of gonorrhoea may cause
neonatal ophthalmia
in babies born to infected mothers. The eyes become infected as the baby passes through the vagina.
Syphilis
This disease is caused by
Treponema pallidum
. There are three clearly marked stages. After an incubation period of several weeks, the
primary sore
(chancre) appears at the site of infection, e.g. the vulva, vagina, perineum, penis or round the mouth. In the female the primary sore may be undetected if it is internal. After several weeks the chancre subsides spontaneously. The
secondary stage
, 3 to 4 months after infection, involves systemic symptoms including lymphadenopathy, skin rashes and mucosal ulceration of the mouth and genital tract. There may then be a latent period of between 3 and 10 years.
Tertiary lesions
(gummas) then develop in many organs, including skin, bone and mucous membranes, and may involve the nervous system, leading to general paralysis and dementia.
Sexual transmission occurs during the primary and secondary stages when discharge from lesions is highly infectious. Congenital transmission from mother to fetus carries a high risk of stillbirth.
Trichomonas vaginalis
These protozoa cause acute vulvovaginitis with irritating, offensive discharge. It is usually sexually transmitted and is commonly present in women with gonorrhoea. Males are often asymptomatic.
Candidiasis
The yeast
Candida albicans
(see also
p. 311
) is frequently a commensal in the normal vagina and causes no problems. It is normally prevented from flourishing by vaginal acidity, but in certain circumstances it proliferates, causing candidiasis (thrush). Common precipitating factors include:
•
antibiotic therapy, which kills the bacteria that keep vaginal pH low
•
pregnancy
•
reduced immune function
•
diabetes mellitus.
In women, persistent itch is the main symptom, with discharge, swelling and erythema of the vulvar area.
Acquired immune deficiency syndrome (AIDS) and hepatitis B infection
These viral conditions may be sexually transmitted, but there are no local signs of infection. For a description of AIDS and HIV see
page 376
and hepatitis B
page 325
.
Non-specific genital infection
This is increasingly common, especially in males. General symptoms include painful urination and urethral discharge, and there is a wide range of possible causative organisms. Some cases are not sexually transmitted and arise from, for example, urinary tract infection or the presence of a foreign body in the urethra.