Pediatric Primary Care Case Studies (73 page)
Read Pediatric Primary Care Case Studies Online
Authors: Catherine E. Burns,Beth Richardson,Cpnp Rn Dns Beth Richardson,Margaret Brady
Tags: #Medical, #Health Care Delivery, #Nursing, #Pediatric & Neonatal, #Pediatrics

Family medical history:
The family consists of Mr. and Mrs. Garcia, Miguel (age 12 years, has mild asthma); Anna (age 10 years, in good health); Ignatio (age 9 years, recently diagnosed with ADHD), and Maria (age 5 years, with a seizure disorder for the past year). The parents are in good health, do not smoke or take medication, and have had no health problems. There is no family medical history of bleeding problems, G6PD, Fanconi anemia, chronic blood problems, autoimmune diseases, gall stone surgery, splenectomy, or heart disease.
Social history:
The family moved to Yakima Valley, Washington, 6 months ago from California to work in the orchards. They had worked in California for a few years in the citrus industry before coming to Washington to be closer to family and to work at the same place year-round. Mrs. Garcia reports that the necklace that Oswaldo wears is a holy medal to keep him safe, which was given to him by his grandmother at his christening. Oswaldo’s mom confides that since his change in activity and appetite, the ladies and parents have been praying to the Virgin for Oswaldo and light many candles. The curandera gave them tea to help Oswaldo, amulets of the Virgin for the Mal de Ojo, and oils to rub in for the “empacho” (Kemp, 2005).
Box 19-1
discusses Mexican/Chicano health practices that may provide insight about their health belief system.
Environmental history:
The family lives in a three-bedroom apartment in the company’s housing complex, which was built just after World War II. The apple orchard and fruit farm where Oswaldo’s father is employed utilizes pesticides, and the workers wear masks when they apply it. Dad does not change clothes before coming home and playing with the children. They recently have had problems with mice in the apartment so the parents put out some rat poison (super warfarin). There has not been any observed contact with the poison by any of the children, but Mrs. Garcia admits that she does not watch each of the children every second. The other children are all doing fine except as noted above.
Box 19–1 Mexican/Chicano Health Practices
• Mexican immigrants are typically Roman Catholic with a spiritualism that also harkens to their Aztec and Mayan predecessors.
• Healers, or
curanderas
, are usually females (mothers, grandmothers) who have learned their healing practices through an ages-old apprenticeship process.
• Prayer is commonly used to help with healing, especially prayer to important saints such as the Virgin of Guadalupe or Our Lady of San Juan.
• Families commonly have shrines in their homes where they lay amulets and light candles.
• When faced with illness, prayer, lighting of candles, wearing of holy medals and amulets, and even pilgrimages to shrines are common practices.
• Herbs, teas, and massage are also commonly employed as cures.
• Health is a matter of balance. The major balance is hot–cold. Belief in the fundamental nature of the hot–cold balance in health regulation may have an influence about what the sick person may eat, what medicine they will take, and when they do. An example of a “cold” illness is
empacho
, which literally translated means an impacted stomach. Anyone can have
empacho
, but it is commonly associated with gastrointestinal illnesses of children. This “cold” illness is said to be caused by soft or hard-to-digest foods adhering to the stomach wall.
• The
curandera
is an integral member of the immigrant’s community with personal ties to the families she treats. Children and their families are not likely to reveal their interactions with these traditional healers until they feel very comfortable with the clinic and the provider.
Sources:
Based on Spector, R. (1996).
Culture and diversity in health and illness
(4th ed.). Stamford, CT: Appleton & Lange; Kemp, C. (2005).
Mexicans and Mexican-Americans: health beliefs and practices
. Retrieved April 10, 2009, from
http://bearspace.baylor.edu/Charles_Kemp/www/hispanic_health.htm
Review of systems:
Because her son sometimes has “crampy stomachaches,” Mrs. Garcia gives him Maltsupex 1 tsp, which she adds to his bottle once or twice per week to help him move his bowels when he seems to have a stomachache. Amoxicillin was completed 2 weeks ago; she denies using herbals or other complementary or alternative medicine (CAM) remedies. Mom has not noticed rashes or lesions except for increased bruising for about a month. When he fusses, which he does more and more lately, he shakes his head and closes his eyes. He seems to focus on objects; his eyes are clear with no redness or discharge. He has had several nosebleeds over the past couple of weeks, which seem to be more frequent the past few days. There is cracking at the corners of his mouth, and his tongue looks redder to his mother than usual but doesn’t seem to hurt him.
There is no history of diarrhea or vomiting; he is still in diapers. Stools are dark clay-like about twice per week. No blood noted in his stools. He is a picky eater, preferring to drink cow’s milk from the bottle, which he carries around with him. As he has gotten thinner and paler, mom has just been happy with whatever he eats. For breakfast he usually eats some
oatmeal and fruit, lunch consists of some vegetables and rice, and dinner is rice and beans or casseroles. There is always fruit to eat at home, which mom washes as soon as she brings it home. Total cow’s milk ingestion is between 32 and 40 ounces per day.
A review of his development reveals that he sat up at 6 months, stood alone at 11 months, is now walking, but lately prefers to crawl again. He said his first word at 12 months, now has 8–10 words in Spanish, puts everything in his mouth, and eats dirt when he plays outside. He plays quietly, preferring more and more to watch others play.
What should you know about the use of Maltsupex?

Maltsupex is commonly used in Mexican American populations for the treatment of constipation. You will address the use of laxatives with Oswaldo as part of your management plan.
Considering the child’s age and developmental stage, what are the most common etiologies for pallor and anemia?
What possible causes for this presentation come immediately to mind?
Acquired pallor in a toddler is unusual and should cause one to think of problems of cutaneous blood flow, anemia, or some unknown mechanism. At 18 months of age, the likelihood of cutaneous blood flow issues is rare; anemia is much more likely. The recent onset of the pallor is more indicative of anemia. Anemia is diagnosed when the hemoglobin concentration (hematocrit) is more than two standard deviations below the mean. Pallor can also occur in association with bleeding, which expands diagnostic possibilities to include leukemia.
Based on the information at hand, what are your priorities for assessment during the physical examination?
There may have been exposure to several environmental toxins—rat poison (blood thinner), pesticides from the orchard transmitted on father’s clothes (neurotoxin), and soil toxins such as lead or pesticides consumed via his pica behavior. The diet is inadequate in iron due to large quantities of milk ingestion and low ingestions of foods high in iron, and the milk ingestion could contribute to his constipation. Oswaldo’s development has regressed slightly, as demonstrated by his now preferring crawling to walking. Oswaldo has become more sedentary and irritable over the past few weeks. Therefore, the neurological, skin and mucus membrane, abdominal, and cardiac examinations will be key areas to evaluate during the physical examination. A developmental assessment will also provide important information.
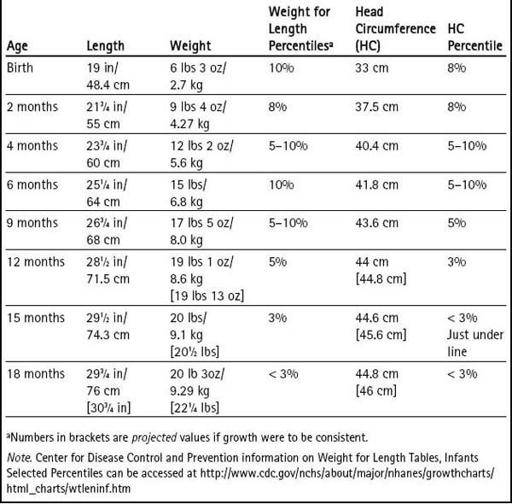
Likewise, the healthcare provider should review his growth chart (see
Table 19-1
), which reveals that his height to weight ratio has stayed around 10% from birth, but over the past 6 months a decline in his growth trajectory is evident by a flattened curve. Currently, height and weight are below the third percentile.
Table 19–1 Measurements from Oswaldo’s Healthcare Visits
Physical Examination
Oswaldo presents as a quiet, attentive, subdued child sitting on mom’s lap without moving around or reaching for toys or other objects. His vital signs are heart rate 112, respiratory rate 24, and height and weight below the third percentile. There are multiple 1 × 1 cm to 2 × 3 cm bruises of varying ages notable on extremities and forehead. Nails are without lesions with a capillary refill of 2 seconds. His anterior fontanel measures 1 × 1 cm and is flat. His ears and nose are within normal limits. The sclera have a bluish tint, and conjunctiva are pale; attempts to visualize fundi were futile. Irritation and cracking are noted at corners of mouth, and his tongue looks red but does not seem to hurt him. The oral mucosa is pale but no dark lines are noted along the gums. His neck, lungs, heart, and musculoskeletal exam are unremarkable. Abdominal exam is positive for palpable stool (left abdomen—midline and lower abdomen) and a palpable spleen 1 cm below the costal margin. His deep tendon reflexes are 2+ bilaterally, and cranial nerves are grossly intact.