Read Pediatric Examination and Board Review Online
Authors: Robert Daum,Jason Canel
Pediatric Examination and Board Review (97 page)

FIGURE 59-1.
Preseptal Cellulitis. Left preseptal cellulitis with edema and erythema of the eyelids. Note that the conjunctiva is clear and not injected. (Reproduced, with permission, from Knoop KJ, Stack LB, Storrow AS, et al. Atlas of Emergency Medicine, 3rd ed. New York: McGraw-Hill; 2010:431. Photo contributor: Kevin J. Knoop, MD, MS.)
2.
(A)
In cases where orbital cellulitis is not suspected, history and physical examination should lead to the correct diagnosis (see
Figure 59-2
). A CBC may be somewhat helpful if a leukocytosis or “left shift” is present, but such a change is nonspecific. A culture of the eye discharge, if present, takes too long to be helpful in immediate decision making. A CT is not indicated for preseptal cellulitis unless orbital involvement cannot be excluded.
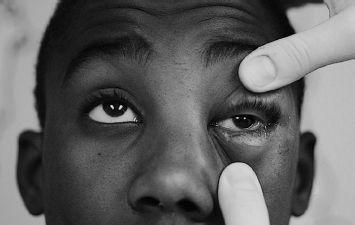
FIGURE 59-2.
Left orbital cellulitis with decreased range of motion secondary to edema. Note the injected conjunctiva. (Reproduced, with permission, from Knoop KJ, Stack LB, Storrow AS, et al. Atlas of Emergency Medicine, 3rd ed. New York: McGraw-Hill; 2010:431. Photo contributor: Javier A. Gonzalez del Rey, MD.)
3.
(D)
Because of the lack of vaccination receipt in this child,
H influenzae
type b should probably still be considered even though it is unlikely. Once a major pathogen causing preseptal cellulitis, it is now quite rare because of the vaccination program against it in the United States. The patient is also 4 years old, on the tail end of what was the
H influenzae
type b agespecific curve.
H influenzae
type b causes a rapidly progressive preseptal cellulitis and therefore it is appropriate to treat presumptively with parenteral antibiotics that cover it as well as the other common causes,
S aureus
,
S pneumoniae,
and
S pyogenes
. Clindamycin is now an agent of choice to cover these gram-positive species in the many areas where methicillin-resistant
S aureus
(MRSA) isolates are prevalent.
4.
(D)
Orbital cellulitis is differentiated from preseptal cellulitis based on anatomy (anterior vs. posterior to the orbital septum), symptomatically (pain on eye motion, decreased vision), and by physical findings (proptosis, decreased extraocular movement).
5.
(A)
Paranasal sinusitis is the most common associated finding with orbital cellulitis in children. Direct extension of infection or venous spread can also occur from the lid, conjunctiva, globe, lacrimal gland, or nasolacrimal sac. Frontal sinusitis also can cause contiguous spread of infection although less frequently than paranasal sinusitis. In addition, because of the age at which sinuses develop anatomically, paranasal sinusitis occurs in a younger group (frontal sinuses begin to develop at approximately 7 years old).
6.
(C)
Although all of the above are implicated, the incidence of
H influenzae
infection has decreased dramatically since widespread vaccination began in 1985. Members of the species other than type b may still found in older children with frontal sinusitis extending to the orbit with resultant cellulitis.
7.
(D)
Although physical examination can often lead to the differentiation between orbital and preseptal cellulitis, a CT of the orbits makes the definitive diagnosis. Orbital CT changes may be minimal, however, in the absence of abscess. CT is superior to MRI in its ability to distinguish the orbital soft tissues from the surrounding bone. Some experts believe that known orbital abscesses can be followed with ultrasound to limit radiation exposure, but this modality is not useful as an initial evaluation.
8.
(D)
He should receive parenteral antibiotics for 7-10 days, depending on the rapidity of improvement. Oral antibiotics may then be used to complete a 21-day course.
9.
(B)
Preseptal cellulitis occurs most often in children younger than 5 years old, whereas orbital cellulitis occurs in older children and, less commonly, adults.
10.
(A)
Whereas orbital cellulitis is commonly an associated finding of sinusitis, preseptal cellulitis is commonly an associated finding of trauma, upper respiratory tract infections, or dacryocystitis.
11.
(B)
Viral conjunctivitis is common during an upper respiratory tract infection. It is more commonly bilateral, watery, and mild to moderate conjunctival injection.
12.
(D)
This is pharyngoconjunctival fever, caused by adenovirus. The diagnostic triad is fever, conjunctivitis, and pharyngitis.
13.
(A)
As opposed to viral conjunctivitis, bacterial conjunctivitis is more often unilateral. There is severe injection and thick and sometimes copious yellow discharge. It often follows a viral upper respiratory tract infection.
14.
(D)
Topical antibiotic drops are the best way to treat bacterial conjunctivitis. The fluoroquinolones are heavily promoted for the therapy of conjunctivitis but select for resistance frequently. Sulfacetamide drops are almost always effective and still constitute relatively inexpensive front-line therapy.
15.
(B)
This is typical nasolacrimal duct (NLD) obstruction that can occur in the newborn period and can be relapsing. It most often resolves by 9-12 months of age. Symptoms include watering and yellow discharge. In the newborn period the conjunctivae are sometimes mildly erythematous, making the differentiation between NLD obstruction and chlamydia or gonococcal infection difficult. In most cases, treatment for NLD obstruction is not provided unless it persists past 9-12 months, at which time therapeutic probing of the NLD can be performed by an ophthalmologist.
16.
(D)
This is a chalazion, a granulomatous inflammation in the meibomian gland (see
Figure 59-3
). These can be chronic, and inflammatory signs are typically absent. Treatment most often is not warranted, although surgical excision may be needed in instances of a large growth obstructing vision.

FIGURE 59-3.
Chalazion. This nontender lowerlid chalazion was seen with lid eversion. (Reproduced, with permission, from Knoop KJ, Stack LB, Storrow AS, et al. Atlas of Emergency Medicine, 3rd ed. New York: McGraw-Hill; 2010:37. Photo contributor: James Dahle, MD.)
17.
(B)
This is most likely an external hordeolum, or stye. Internal hordeolums are on the inner lid and appear to be bulging from underneath. Dacryocystitis, or infection of the lacrimal gland, is located inferiorly and medially to the medial tear duct. Blepharitis is inflammation of the lid margins and typically has erythema and crusting or scaling.
18.
(C)
Amblyopia may occur as a result of ptosis, either from the lid covering the visual axis or astigmatism secondary to the weight of the lid on the globe.
 S
S
UGGESTED
R
EADING
Behrman RE, Kliegman RM, Jenson HB, et al.
Nelson Textbook of Pediatrics
. Philadelphia, PA: WB Saunders; 2007.
Greenberg MF. The red eye in childhood.
Pediatr Clin North Am.
2003;50(1):105-124.
Mawn LA. Preseptal and orbital cellulitis.
Ophthalmol Clin North Am.
2000;13(4):633-641.
CASE 60: A 9-MONTH-OLD IN A CAR ACCIDENT
You see a 9-month-old infant in the emergency department with his mother, who was rear-ended in a car accident 1 hour prior. At the time of the accident, he was in his infant carrier car seat, in the backseat, facing forward. Since that time he has been acting his usual self, smiling and laughing, playful, and hungry.
On examination, he weighs 22 pounds, is alert, and interactive. His neurologic examination is normal, as is the rest of his examination.
SELECT THE ONE BEST ANSWER
1.
What can you tell his mother about his car seat?
(A) it should be forward-facing in the front seat
(B) it should be rear-facing in the front seat
(C) it should be forward-facing in the backseat
(D) it should be rear-facing in the backseat
(E) he should be in a booster seat
2.
She is wondering if the airbags in her 4-door car are a danger to him while he is restrained in his car seat. What will you tell her?
