Pediatric Examination and Board Review (190 page)
Read Pediatric Examination and Board Review Online
Authors: Robert Daum,Jason Canel

Long SS, Edwards KM. Prolonged, recurrent, and periodic fever syndromes. In: Long SS, Pickering LK, Prober CG, eds.
Principles and Practices of Infectious Disease.
3rd ed. Philadelphia, PA: Churchill Livingstone; 2008:126.
Shapiro ED. Lyme disease.
Pediatr Rev.
1998;19:147-154.
Chapter 13
NEGLECT AND ABUSE
CASE 107: A 4-MONTH-OLD WITH WEIGHT LOSS
A 4-month-old boy is brought to the emergency department for evaluation of a cough and a tactile fever. On examination the patient is afebrile and has upper airway congestion, but you immediately note that this child appears small for his age, malnourished with loss of subcutaneous fat, and has an erythematous candidalappearing diaper rash. The baby is alert, follows well, and appears to have appropriate tone.
The mother states she has been concerned about her infant’s small size and has brought her baby to the doctor requesting advice to help her baby grow, but she has not seen a physician in 4 weeks. The child has been fed standard formula mixed appropriately by the mother since birth, and according to the mother the child is a good eater.
The mother is 34 years old and has 2 other children at home who are well; both are in school and according to the mother have no growth problems. You measure the child’s weight, head circumference and height, and you plot the values on a growth curve (see
Figures 107-1
and
107-2
).
SELECT THE ONE BEST ANSWER
1.
You are concerned about this baby’s current state of malnutrition. Your immediate plan is to
(A) review the past medical history, inquire about risk factors for immune system disorders, and perform screening tests. You also ask the mother to keep a calorie calendar of daily input and plan to see her and her infant next week
(B) order a screening complete blood count (CBC), metabolic panel, pre-albumin, albumin, ferritin, thyroid-stimulating hormone (TSH), and a home visiting health nurse for dietary education and weight assessment
(C) admit your patient to the hospital for evaluation
(D) send the child home because your presumptive diagnosis is intrauterine growth retardation because of the symmetry of the growth failure, and you change the child’s formula to an increased calorie per ounce formula
(E) send the child for a genetics consultation
2.
To assess this child’s growth, what would be the next important step?
(A) obtain consent from the mother to review the patient’s medical record and growth chart from her pediatrician
(B) measure the pre-albumin, ferritin, and place a Mantoux test
(C) obtain a bone age radiograph
(D) obtain the sibling’s growth charts
(E) obtain electrolytes with a complete metabolic panel to assess for hydration
3.
You are able to obtain your patient’s prior growth measurements from his pediatrician, and you find the following: birth weight, length, and head circumference were all at the 50th percentile. Only one subsequent visit occurred at 2 months of age when the child was between the 10th and 25th percentiles on the growth chart. True statements regarding growth parameters include the following except
(A) weight for age reflects multiple factors including current and past growth problems
(B) depressed weight for height reflects more acute nutritional deprivation
(C) a depressed height reflects chronic malnutrition
(D) adjustments for prematurity are unnecessary past 1 year of age
(E) assessing the grade of nutrition guides both management and intervention
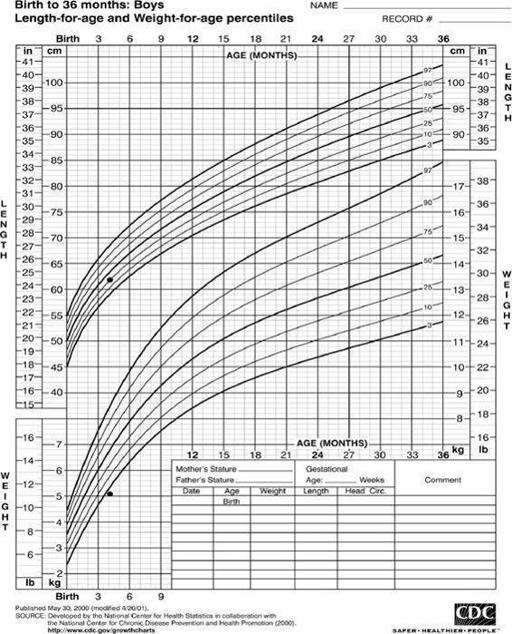
FIGURE 107-1.
Growth charts of 4-month-old infant with weight loss.
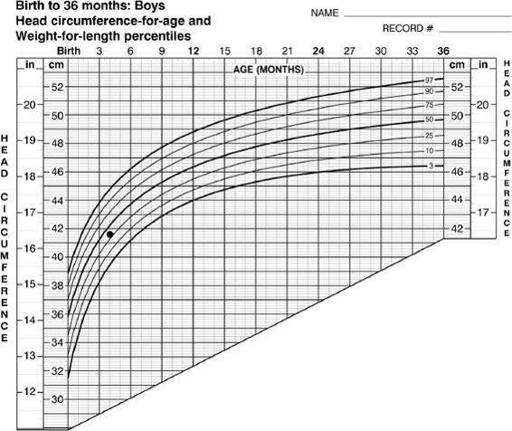
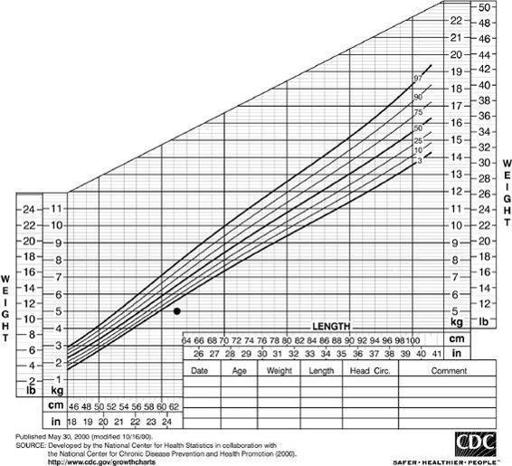
FIGURE 107-2.
Growth charts of 4-month-old infant with weight loss.
4.
True statements regarding examination and laboratory evaluation for children with failure to thrive (FTT) include all of the following except
(A) all children with FTT should have baseline metabolic evaluation, human immunodeficiency virus (HIV) testing, sweat test, thyroid studies, screening electrocardiogram (ECG), and stool for parasites
(B) short children should have a bone age performed
(C) the physical examination aids in identifying findings suggestive of chronic illnesses and potentially growth-retarding syndromes
(D) laboratory testing is guided by history and physical examination
(E) evaluation for gastrointestinal (GI) abnormalities should be considered in children with unexplained vomiting
5.
True statements regarding FTT management include all but the following
(A) ensuring appropriate nutrition for a child with FTT incorporates both catch-up and maintenance nutrition
(B) the amount of expected growth of a normal child varies with age
(C) heavy prenatal exposure to alcohol is associated with microcephaly and short stature
(D) demonstrating growth with provision of adequate nutrition in the hospital suggests a diagnosis of “nonorganic” FTT
(E) optimizing management includes an interdisciplinary approach, daily intake evaluation, and integration of the family in understanding the goal of a hospital admission for an FTT evaluation
6.
Parental competency is affected by all of the family characteristics except
(A) parental resources
(B) maternal mental health
(C) lack of college education
(D) child characteristics
(E) family social context
7.
The most common form of child maltreatment is
(A) physical abuse
(B) sexual abuse
(C) infanticide
(D) neglect
(E) lack of supervision
8.
The number of annual reports made nationally to a child abuse hotline is
(A) 60,000
(B) 1 million
(C) 2 million
(D) 3 million
(E) 5 million
9.
During your evaluation of the child with FTT, you find out that the mother has just moved into a domestic violence shelter and discloses that up until this recent move, her partner had been limiting her ability to purchase food and access medical care for her baby. During the hospitalization the mother is engaging the child and the child takes nutrition well from the mother. She has just obtained a protective order from the courts with regard to her partner. All of the following are true except
(A) in some jurisdictions the only access to necessary services for this mother is through a child welfare referral
(B) all children with FTT are required by law to be reported to child welfare services
(C) protective service intervention with placement of the child out of the home may be necessary in noncompliant family situations to enhance medical compliance
(D) referral to a child protection agency is warranted when safety cannot be ensured in the current environment
(E) foster care placement has a potential for suboptimal placement
10.
The most common risk factor for FTT in a child is
(A) maternal depression
(B) poverty
(C) prematurity
(D) poor oral motor skills
(E) maternal drug use
11.
A skeletal survey is performed and a healing clavicle fracture is found. The following is a true statement
(A) the finding of a fracture on the skeletal survey is diagnostic of child abuse
(B) clavicular fractures in toddlers are rare and should raise suspicion of child abuse
(C) because of the finding of a clavicular fracture, a computed tomography (CT) of the head and ophthalmologic examination should be ordered