Read Oxford Handbook of Midwifery Online
Authors: Janet Medforth,Sue Battersby,Maggie Evans,Beverley Marsh,Angela Walker
Oxford Handbook of Midwifery (65 page)

- Stretch receptors in the vagina, rectum and perineum communicate changes in volume, tension, and tone, possibly accounting for the complexity of symptoms experienced at the transition stage.
- Passive descent should be allowed until the fetal head becomes visible.
There is scant evidence to suggest that active pushing in the latent phase of the second stage achieves much other than exhausting and discouraging the mother.
Early physical and auditory signs of the active second stage
- If the membranes are intact, they will commonly rupture at full dilatation.
- The woman has a sensation of wanting to have her bowels open during a contraction.
- A bright red loss may be observed.
- The woman shows renewed strength and excitement, and ability to work with her contractions.
- A purple line may appear, extending from the anus to the nape of the buttocks. It is not recognizable in all women, due to obesity or upright positions.
1 - The woman may grunt at the height of a contraction and show facial congestion during pushing efforts.
Advanced signs of the second stage
- Vulval and perineal areas bulge and gape.
- The anus pouts and then flattens. The woman may empty her bowels during a contraction.
Active phase: physiology
- The urge to push allows the presenting part to descend to compress the tissues of the pelvic floor.
- Approximately 1cm above the ischial spines, pressure from the fetal presentation stimulates nerve receptors in the pelvic floor (Ferguson’s reflex) and an uncontrollable urge to bear down is experienced.
- During expulsive contractions, muscle fibres of the vagina and uterus draw up and tighten the lining of the birth canal, providing a taut surface against which the presenting part can slide down.
- Beynon’s (coat/sleeve) analogy. When an arm is quickly put in a coat sleeve, the lining is dragged out with hand; if the lining is held at the top everything stays in place. In childbirth, when told to push immediately at the beginning of a contraction, the pulling up mechanism may be
diminished or prevented, leading to delay or damage.

- Odent
2
identifies the ‘fetal ejection reflex’ when there is a steep rise in the release of catecholamines during the last few contractions before birth. This is recognized by the woman suddenly becoming more alert and energized. She may need to drink a glass of water and perhaps hold on to someone. This ensures that the woman is alert and therefore protective for when the baby is born. The fetus also releases its own catecholamines at this time and is observed in the wide eyed, alert baby who gazes at its mother directly after birth.CHAPTER 14
Normal labour: second stage268
Contractions of the second stage
Contraction alone = 70–80mmHg
+
Extra surges at peak of contraction = 70–80mmHg Therefore total effort = 140–160mmHg
Stretch receptors and pushing
Stretch receptors are activated in the wall of the vagina, rectum, and peri- neum, especially during the surges of the contractions:
Uterine surges + abdominal pressure + receptors = overwhelming desire to push
Recommended reading
Downe S (2009). Transition and the second stage of labour. In: Fraser D, Cooper A (eds)
Myles Textbook for Midwives
, 15th edn. Edinburgh: Churchill Livingstone.
- Hobbs L (1998). Assessing cervical dilatation without VEs.
Practising Midwife
1
(11), 34–5. - Odent M (2001). New reasons and new ways to study birth physiology.
International Journal of Gynecology and Obstetrics
75
Suppl 1, S39–S45.
This page intentionally left blank
CHAPTER 14
Normal labour: second stage270
Mechanism of labour
During labour the fetus makes a series of passive movements, collectively known as the mechanism of labour (Fig.14.1). These enable the fetus to adapt to the changes of the pelvis and birth canal, making use of the best space available. It is important to have a sound understanding of this mechanism, so that the normal manoeuvres of the fetus at delivery are anticipated and situations when assist- ance may be necessary recognized. This is best depicted diagrammatically.
- Descent commences before labour begins in the primigravidae; in multigravidae this may not occur until labour is established. Further descent is facilitated during labour, particularly during the second stage, when auxiliary muscles (diaphragm and abdominals) are employed to aid expulsion.
- Flexion is the natural attitude of the fetal head at commencement of labour. Flexion becomes more marked as labour progresses. Resistance of the birth canal exerts pressure through the occiput.

Fig. 14.1a
First stage of labour. The cervix dilates. After full dilatation the head flexes further and descends further into the pelvis. - Internal rotation occurs when the occiput (or whichever denominator meets the pelvic floor first) meets the resistance of the pelvic floor, rotating through one-eighth of a circle. The contour of the pelvic floor assists by presenting the longest diameter of the pelvic outlet (antero- posterior diameter). The occiput is then able to escape under the pubic arch and crowning takes place.
- Crowning of the head occurs when it has emerged under the pubic arch and does not recede between contractions. The widest diameter
 of the head (biparietal) is apparent.
of the head (biparietal) is apparent. - Extension of the head takes place to facilitate the bregma, forehead,
face, and chin to sweep the perineum and accommodate the changed contour of the pelvis.
- Following birth of the head, restitution (untwisting of the fetal head) takes place to enable realignment of the head and shoulders, in preparation for delivery of the shoulders and body.
- The shoulders then undergo internal rotation, lying in the antero- posterior diameter of the outlet, to follow the direction of restitution.
MECHANISM OF LABOUR
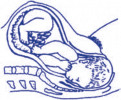
Fig. 14.1b
During the early second stage the head rotates at the levels of the ischial spine so the occiput lies in the anterior part of pelvis. In late second stage the head broaches the vulval ring (crowning) and the perineum stretches over the head.271

Fig. 14.1c
The head is born. The shoulders still lie transversely in the midpelvis.

Fig. 14.1d
Birth of the anterior shoulder. The shoulders rotate to lie in the antero- posterior diameter of the pelvic outlet. The head rotates externally, ‘restitutes’, to its direction at onset of labour.CHAPTER 14
Normal labour: second stage272
- The anterior shoulder is then born by applying gentle downward traction. The posterior shoulder and trunk are then born by lateral flexion. If traction is not applied, it is not uncommon for the posterior shoulder to be born first.

Fig. 14.1e
Birth of the posterior shoulder.
This page intentionally left blank
CHAPTER 14
Normal labour: second stage274
Principles of care in the second stage of labour
The second stage of labour places extra emotional and physical demands on the woman. Extra vigilance is required in terms of midwifery care and support.
- Vital signs
. In normal labour unnecessary recordings of the blood pressure (BP) and pulse will hinder the woman’s concentration and focus. She may be affected by pain, anxiety, fear, and contractions, therefore taking the BP is of minimal value when the woman is actively pushing. Ausculate the fetal heart every 5min and between contractions in the latter part of the second stage. - Contractions
. Note frequency, strength, and length. Identify the different phases of the second stage—strong expulsive contractions for the active phase. - Vaginal loss
. Observe amniotic fluid or blood loss. Be aware of any abnormalities. - Bladder
. Encourage the woman to empty her bladder at commencement of the second stage. Failure to do this can lead to delay and trauma to the bladder at delivery. - Cleanliness and comfort
. Due to the woman’s extra physical efforts and emotional strain, it may help to:- Sponge her face, or use a fine water spray/mister
- Sponge her hands, neck, and arms
- Give her sips of iced water or mouthwash between contractions
- Have a fan in room if it is hot
- Give her simple massage, particularly if she is prone to cramp
- Give her physical support during contractions
- Clean/swab her vulval area and provide a clean pad as frequently as required
- Use complementary therapies if she wishes
- Explore positions for comfort and to assist with the birth—an upright position will aid descent of the fetus and give the woman more control over the process
- Play music if she wishes
- Encourage her to use breathing awareness
- Encourage the involvement of her birth partner.
- Sponge her face, or use a fine water spray/mister
- Hobbs L (1998). Assessing cervical dilatation without VEs.
Other books
The Piper by Lynn Hightower
Nazis in the Metro by Didier Daeninckx
Every Man in This Village Is a Liar: An Education in War by Megan K. Stack
The Man Who Sees Ghosts by Friedrich von Schiller
Tequila Truth by Mari Carr
Wading Home: A Novel of New Orleans by Rosalyn Story
In the Hour Before Midnight by Jack Higgins
My First Seven Years (Plus a Few More) by Dario Fo
Men Who Love Men by William J. Mann
The Alpine Betrayal by Mary Daheim
