Gulp: Adventures on the Alimentary Canal (34 page)
Read Gulp: Adventures on the Alimentary Canal Online
Authors: Mary Roach
Tags: #Science, #Life Sciences, #Anatomy & Physiology

Sydenham did not explain himself. I was left wondering whether this was an early form of animal-assisted therapy and the kitten’s role was simply to help the patient relax while nature took its course. Impactions often resolve on their own. Sydenham once treated an overburdened London businessman by sending him to Edinburgh to visit a specialist who didn’t exist. The patient returned from his weeklong rail journey vexed but rested and cured.
It’s also possible, though unlikely, that the kneading of the kitten’s paws was viewed as a kind of therapeutic massage. Around the turn of the last century, massage—or medical gymnastics, as it was also then called—was not uncommonly applied to the obstructed bowel. Here is Anders Gustaf Wide, in the
HandBook of Medical and Orthopedic Gymnastics
, discussing the technique of “colon-stroking”: “One can at least feel the lower part of the larger intestine and often the hard feces in it and even feel, how, in stroking, these are carried forward in the direction they should go.”
Or not. In a 1992 University of Munich study, nine sessions of “colonic massage” failed to speed colon transit time in constipated subjects and nonconstipated controls. The subjects’ sense of well-being was monitored throughout the three weeks of treatment, and this too failed to improve. It might have gone differently had the masseuses incorporated some techniques from Anders Gustaf Wide—“anal massage,” for instance, wherein “small circular strokings are made to each side alternately with tremble-shaking round the anus.”
Surgeons, too, advocated the use of the hands to dislodge an impaction, though here it was less of a laying-on than a reaching-in. “I propose this evening to demonstrate upon the cadaver some phases of bowel exploration,” began our friend W. W. Dawson, the professor of surgery from the Medical College of Ohio, whom we met in a previous chapter. The year was 1885. Dawson introduced his assistant, Dr. Coffman, to the gathered crowd and then turned to face the examining table. “The subject, you see, is a female.” We’re going to skip ahead to item 2 on the agenda: “How far can the hand be introduced?” The “patient” was rolled on her back with the thighs raised and the knees bent. The position is known as the lithotomy position, or the missionary position, depending on whether you are taking things out or putting them in. In this case, it was a bit of both. “Dr. Coffman now introduces his hand through the anus and presses gently onward and upward.” Here Dawson invited the spectators to watch closely, because it was possible to see the bulge of Coffman’s hand moving below the body’s surface, like a cartoon mole tunneling under the lawn. “Dr. Coffman is able to move his hand with great freedom. You will recognize at once how it would be possible to dislodge . . . impacted feces.”
*
For the most part, the historical treatment of obstructed bowels took its cues from the world of plumbing. There were, as there are with bathroom pipes, two main strategies: blast it free with water or air (plunge it), or break it up with something metal (snake it). The June 1874
Atlanta Medical and Surgical Journal
describes Dr. Robert Battey’s “safe and ready” method of dissolving “accumulations of hardened feces” by injecting water, as much as three gallons, up the rectum. “So great was the abdominal tension that the water spouted from the anus when pressure was removed,” writes Battey of one memorable case, “in a bold stream” two feet high. Battey’s lecture was accompanied by a demonstration. A haphazard perusal of the medical journals of the day seemed to indicate, among surgery and anatomy professors, a keen spirit of one-upsmanship that drove lecture hall demonstrations ever farther in the direction of spectacle.
The digestive tract is an intricate, flexuous pipe not easily snaked. Patients had to more or less swallow the snake. For more than a hundred years, swallowing lead shot or metallic mercury, as much as seven pounds, was thought to be a good way to break up an obstruction. The patient was then rolled or shaken, in hopes that the heavy stuff would work its way through the clog. The problem was that the stomach releases its contents gradually, no matter how swiftly they’re swallowed. Rather than pushing through the gut in a cohesive front, the metal shot would journey forth in dribs and drabs, appearing on X-rays like an ingested strand of pearls. Just as well. A physician named Pillore, writing in 1776, describes an autopsy he performed on a patient whose small intestine was so weighed down by the two pounds of mercury that had collected in a lump, that a loop of the organ had stretched and sunk down into the pelvis. The man died a month later. Between the mercury, the unresolved obstruction, and the taffy-pulled gut, it’s anyone’s guess what ultimately did him in.
For a brief span of years, the plumbers stepped aside and the electricians got to work. Like radioactivity in its day, electricity was new and exciting and presumed to cure whatever ailed a person. Galvanic therapy for obstinate constipation—or “obstipation”—entailed passing a mild electrical current through the abdomen. “Efficacious?” an 1871
British Medical Journal
contributor is quoted in reply to a dubious colleague. “I could hardly get out of the way in time.”
The crudest approach to breaking the dam was simply to toss the patient over a hospital attendant’s shoulder.
*
The intestines do not take a fixed position in the human interior, and simple inversion can, in some cases, bring a measure of relief. A Dr. William Lewitt, of Rush Medical College, in 1864 related the case of a man with a tumor in his abdomen the size of “a child’s head at term,” which was putting the squeeze on his digestive works. “On visiting the patient, we found him suffering intense agony from pain in the abdomen, with frequent desire to expel flatus from the rectum, which could only be accomplished by standing upon his head and hands, in a perpendicular position.” Dr. Lewitt gave his title as Demonstrator of Anatomy, and I imagine it took all the restraint he had not to pack the man up and bring him down to the lecture hall for a demonstration.
The treatment of last resort was surgery. If a blockage could not be shaken, stroked, hosed, or zapped into submission, it was likely to be excised. Surgery in the pre-handwashing, pre-glove-donning era bore a sobering risk of infection. Surgery on the bacteria-laden colon, all the more so. Horrifyingly, colectomy was being performed not just for life-threatening impactions, but as a treatment for constipation and its spurious consequence: autointoxication. What better way to speed digesta through the body than by shortening the chute? Scottish surgeon Sir Arbuthnot Lane, the operation’s inventor and vociferous champion, began with “short circuits,” removing a span of a couple feet. Soon he moved on to total colectomy, removing basically healthy colons and stitching the end of the small intestine directly to the rectum. If diarrhea can be considered a cure for constipation, he may have done his job, but in the process he put his patients at risk of nutritional deficiencies. As we learned from the coprophagic rodents of chapter 15, the colon—via the metabolic labors of its bacteria—produces not just feculant putridity, but valuable fatty acids and vitamins.
Lane was a raging coprophobe. The normal variances of skin color that you or I would attribute to race or time spent in the sun, Lane perceived as staining from fecally poisoned blood. One patient’s “yellowish-brown complexion” disappeared, he noted with pride, a month after her surgery. “She has lost almost all her brown colour,” he wrote of another woman. Lane went so far as to deem the colon a useless structure and a “serious defect in our anatomy.”
It takes a sizable sum of arrogance and ignorance to second-guess human anatomy and the evolutionary fine-tuning that produced it. The colon that Lane would so cavalierly lop from his patients’ interiors is more than a simple waste-storage facility. The bacteria feared and despised by the likes of Lane and Tyrrell and Kellogg—the germs that live and thrive and ply their trade within our waste—are not only harmless, they are critical to good health.
*
This was less exciting than it sounds because Dhody keeps the “creepy-tastic” stuff out on display. For example, the necklace of dried hemorrhoids, and the jar of skin (dropped off by the roommate of a compulsive picker, in a Trader Joe’s strawberry preserves jar with a note attached: “Please recycle,” presumably referring to the jar).
*
Oddly, the exhibit chosen for billboarding on the building’s exterior was “Young Women Basketball Players.”
*
It’s amber. Because there are more cancers than colors, awareness ribbons are like paint chips now: Stomach cancer is periwinkle, ovarian is teal. Colon and rectal cancer are plain blue. They used to be brown (just as the color for bladder cancer awareness is yellow), but some patients objected. A mistake, I say. They could have had brown all to themselves; blue they have to share with Epstein-Barr, osteogenesis imperfecta, victims of hurricane Katrina, drunk driving, acute respiratory distress syndrome, child abuse, baldness, and secondhand smoke.
*
He wrote a book on the topic, called
Why Can’t I Go?,
which features dozens of defecography stills and close-ups of colon surgery graphic enough that the back cover has a warning. Can I Go Now?
*
Vigorous debate followed, under the italicized heading “Size of the Hand.” A hand more than nine inches around is, declares Dr. Charles Kelsey, “unfit for the purpose.” Dawson counters that the size of the pelvis must be taken into consideration. “A broad hipped man or woman would admit a ten inch hand readily,” and to fix the limits lower would have the effect of “deterring and embarrassing the practitioner who happens to have a large hand.” Or four. Dawson also relates the story of a Dr. Cloquet who, “in quest of a glass tumbler,” inserted fourteen fingers into a rectum: six of his own, and four belonging to each of two colleagues. The patient’s sphincter, if not his dignity, recovered intact.
*
In related matters: Is it possible to literally knock the shit out of someone? Depends on the shit and who’s knocking it. “I had a high school football coach who was an offensive tackle for the Washington Redskins,” says gastroenterologist Mike Jones. “He swore to me that Mean Joe Greene hit him so hard he had to go change his pants.” Jones added that his coach had had “a bit of the squirts” at the time, and that it would be tough to hit someone hard enough to “knock a solid turd out of him” and not simultaneously kill him.
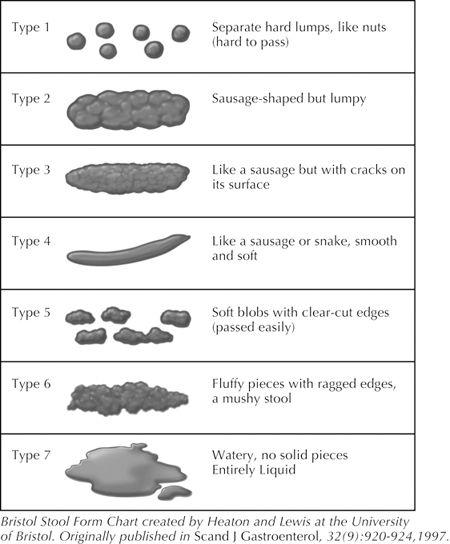
Bristol Stool Chart
WE CAN CURE YOU, BUT THERE’S JUST ONE THING

I
T IS A
standard party invitation in most respects. There’s a street map of the neighborhood, the address and time of the party, and some friendly encouragement to bring the whole family. The decorative elements, though, are unusual: a cutaway illustration of the interior of the human colon, its parts neatly labeled. Above this, in a festive typeface, it says, “Gut Microflora Party!” The host is Alexander Khoruts, a gastroenterologist and associate professor of medicine at the University of Minnesota. Along with the usual complement of colonoscopies and dyspepsia consults, he performs transplants of colon bacteria—aka gut microflora.
Almost everyone gathered at the party this evening is involved with this work. There is Mike Sadowsky, coeditor of the textbook
The Fecal Bacteria
and Khoruts’s research partner. Leaning into the buffet is Matt Hamilton, a University of Minnesota postdoc student who prepares the matter for transplant. Matt is spooning Khoruts’s homemade Russian red beet salad onto a plate, enough of it that a nurse tells him he’s going to “look like a GI bleed” tomorrow.