Breast Imaging: A Core Review (31 page)
Read Breast Imaging: A Core Review Online
Authors: Biren A. Shah,Sabala Mandava
Tags: #Medical, #Radiology; Radiotherapy & Nuclear Medicine, #Radiology & Nuclear Medicine

Reference: Lam WW, Chu WC, Tse GM, et al. Sonographic appearance of mucinous carcinoma of the breast.
AJR Am J Roentgenol
2004;182(4):1069–1074.
49
Answer E.
The images are both STIR (water and fat suppressed) sequences that highlight silicone. The coronal and sagittal STIR sequences both demonstrate intracapsular rupture as evidenced by the presence of the “subcapsular line sign.” This is one of the signs of intracapsular rupture. Loss of integrity of the silicone elastomer implant shell has caused silicone to extend outside the implant shell and become located between the fibrous capsule and the implant shell. Another earlier sign of intracapsular rupture is the “keyhole” sign, which is also known as the noose or lasso sign. Keyhole sign results from a mild loss of integrity of the implant shell that results in small amounts of silicone gel to extend outside the implant shell and become trapped within the folds of the implant. Another sign of intracapsular rupture is the “linguine” sign, which represents more advanced degradation. The implant shell becomes collapsed within the silicone gel and is seen as stacked hypointense lines within the high signal silicone gel. In these examples of intracapsular rupture, the silicone gel is still contained within the fibrous capsule. When silicone extends outside the fibrous capsule, it is known as extracapsular rupture. The provided example demonstrates extracapsular rupture as evidenced by the presence of bright signaled silicone in the breast tissue on the superior aspect of the implant. Answer choices A and C are not correct by themselves, because both of the types of rupture are present. Answer choice B is not correct because the implant is not intact. Subcapsular line sign is present, indicating the presence of intracapsular rupture. A radial fold is a normal infolding (with no intervening silicone gel) of the silicone implant shell in an intact implant. Occasionally, complex radial folds are difficult to distinguish from intracapsular rupture. Actively scrolling through the examination and evaluating the implant in multiple planes can assist with the proper diagnosis. Answer choice D is not correct. Gel bleed is the transudation of microscopic amounts of silicone gel through an intact implant shell.
Reference: Liberman L, Berg WA. Magnetic resonance imaging in women with breast implants. In: Liberman L, Morris EA, eds. Breast MRI:
Diagnosis and Intervention
. New York, NY: Springer Science; 2005:238–265.
50a
Answer E.
This finding is suspicious; BI-RADS category 4. It is a new enhancing irregular mass in a high-risk patient and is therefore considered suspicious by MRI.
50b
Answer B.
The next most appropriate step is focused ultrasound or mammography. Since the finding is suspicious, a recommendation for 6 month follow-up (A) is not appropriate because this finding has a higher than 2% chance of being breast cancer. A recommendation for annual screening breast MRI (C) is similarly inappropriate. Although the finding may result in an MRI-guided breast biopsy (D), an initial attempt should be made to call the patient back for focused ultrasound or mammography for biopsy planning purposes. This additional “second-look” imaging may identify a potential correlate to the MRI finding and the resultant ultrasound or stereotactic breast biopsy is generally a more tolerable biopsy modality. Repeat breast MRI (E) will not be helpful in this instance and is not a sensible use of resources.
51a
Answer C.
51b
Answer B.
The images show an abrupt filling defect immediate past the tip of the 30-gauge blunt-tipped sialogram needle. A filling defect, an abrupt duct cut-off, or luminal irregularity and distortion on galactography are considered a positive study which could be due to
• Intracystic papilloma (most common mass producing a bloody nipple discharge)
• Intraductal papillary carcinoma
• Blood clot
• Inspissated material
• Air bubble
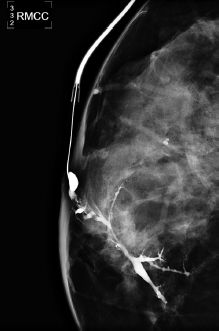
The clinical indications for galactography are single-duct spontaneous bloody, serous, or clear nipple discharge. Procedural steps for galactography are:
Obtain informed written consent.
Breast placed on magnification stand (or patient placed in supine position) with gooseneck light positioned to illuminate the nipple.
Nipple is cleansed.
Duct opening is identified by squeezing nipple to express a small drop of nipple discharge.
The cannula is connected to the tubing and syringe containing 1 to 3 mL of Optiray contrast.
A blunt (27- or 30-gauge), straight or right-angle cannula, connected to tubing and a contrast-filled syringe, is inserted into the duct opening.
The cannula is taped in place to the patient’s breast.
Contrast is injected slowly into the duct until the patient feels fullness in her breast or there is reflux of contrast from the duct.
• Special attention is made not to inject air into the duct, as it can mimic a filling defect on mammogram.
• If resistance occurs while injecting, it may be the result of the cannula being placed against the wall of the duct or extravasation of contrast outside of the duct. Stop injection, and reposition cannula.
Once contrast has been injected, a magnification craniocaudal and lateral view is obtained.
Images are assessed for a filling defect within the duct or abrupt termination of the duct. Both findings will require biopsy.
Galactography can assess for a mass within or compromising a duct, but cannot differentiate benign or malignant etiology.
References: Ikeda D.
Breast Imaging: The Requisites
. 2nd ed. St. Louis, MO: Elsevier Mosby; 2011:383–389.
Shah BA, Fundaro GM, Mandava S.
Breast Imaging Review: A Quick Guide to Essential Diagnoses
. 1st ed. New York, NY: Springer; 2010:231–234.
52
Answer A.
Study is incomplete. Additional imaging evaluation is recommended. Although bilateral similar-appearing masses are considered benign, the patient presented with a palpable lump. Complete diagnostic workup of a palpable lump would include an ultrasound of the palpable area.
Reference: Parikh JR, Bassett LE, Mahoney MC, et al.
Expert Panel on Breast Imaging. ACR Appropriateness Criteria Palpable Breast Masses
. Reston, VA: American College of Radiology; 2009.
http://www.acr.org/~/media/ACR/Documents/AppCriteria/Diagnostic/PalpableBreastMasses.pdf
, Accessed August 31, 2012.
53
Answer B.
Radial scars are not truly scars. Instead they are idiopathic entities unrelated to prior surgery or trauma. Proposed possible causes include localized inflammatory reaction and chronic ischemia with subsequent slow infarction. The prevalence is 0.1 to 2 per 1,000 mammograms. Their major clinical significance pertains to an association with ADH and carcinoma that is seen in up to 50% of cases.
Reference: Alleva DQ, Smetherman DH, Far GH Jr, et al. Radial scar of the breast: Radiologic pathologic correlation in 22 cases.
Radiographics
1999;19:S27–S35.
54
Answer C.
This is a hematoma. Short term follow up is usually performed to assess resolution because it can often mimic a malignancy.
55
Answer D.
The finding of ADH at needle biopsy raises concern about concomitant presence of carcinoma in the lesion sampled by the needle. The incidence of coexistent DCIS or invasive carcinoma is about 20% to 25%. For this reason, a diagnosis of ADH on stereotactic core biopsy is an indication of surgical excision.
Reference: Eby PR, Ochsner JE, DeMartini WB, et al. Frequency and upgrade rates of ADH diagnosed at stereotactic vacuum assisted core biopsy.
AJR Am J Roentgenol
2009;192(1):229–234.
56
Answer D.
Fibrocystic change is more common in patients older than 30 years. The cysts originate from terminal lobules. They appear anechoic on ultrasound, and have high T2 signal intensity, and without enhancement or thick peripheral enhancement on MRI. The fluctuation of the size of the cysts is common.
Reference: Ikeda DM.
The Requisites: Breast Imaging
. 2nd ed. St. Louis, MO: Elsevier Mosby; 2011:62–70, 198–205.
57
Answer A.
The most common pleural presentation of breast cancer is malignant pleural effusion. In fact, thoracentesis with cytology can be performed to help diagnose metastatic disease.
Reference: Banerjee AK, Willetts I, Robertson JF, et al. Pleural effusion in breast cancer: A review of the Nottingham experience.
Eur J Surg Oncol
1994;20(1):33–36.
58
Answer C.
Although radial scar is a benign proliferative breast lesion, it cannot be differentiated from breast cancer with mammography and frequently requires biopsy. It may contain or be associated with atypical ductal hyperplasia or low-grade DCIS, and therefore, surgical excision is needed.
Reference: Ikeda DM.
The Requisites: Breast Imaging
. 2nd ed. St. Louis, MO: Elsevier Mosby; 2011:99, 103.
59
Answer C.
Features suggesting malignancy on breast MRI include bright enhancement, spiculated margins, rim enhancement (beware of fat necrosis and inflamed cyst that can do this), heterogeneous enhancement, enhancing septations, ductal/linear-branching/segmental enhancement, associated enhancement of adjacent tissue region, enlarged feeding blood vessel.
Reference: Ikeda DM.
The Requisites: Breast Imaging
. 2nd ed. St. Louis, MO: Elsevier Mosby; 2011:250–253.
60
Answer D.
Phyllodes tumor has a spectrum from benign to borderline to malignant. Typical presentation is large and rapidly growing in size (more than 20% increase in diameter in 6 months). Typically, they do not have calcifications. The median age is 45 to 49 years, with 21% risk of recurrence mostly within the first 2 years of excision. Radiation therapy reduces the risk of recurrence, and surgical excision is usually curative.
Reference: Ikeda DM.
The Requisites: Breast Imaging
. 2nd ed. St. Louis, MO: Elsevier Mosby; 2011:110–114.
61
Answer C.
Male breast cancer is mostly sporadic and most commonly presents in the upper outer quadrant or subareolar region eccentric to the nipple in the upper outer quadrant. Majority of the male breast carcinoma is invasive ductal carcinoma (IDC), which associated DCIS in 35% to 50% of the time. Pure DCIS is only 7% to 11%.
Reference: Ikeda DM.
The Requisites: Breast Imaging
. 2nd ed. St. Louis, MO: Elsevier Mosby; 2011:279–287.
62a
Answer D.
62b
Answer A.
Rolled views are useful for determining the location of a lesion seen only in the CC projection. The top of the breast can be rolled laterally or medially, and the technologist should label the image appropriately to indicate which way the breast was rolled (CC RL and CC RM, respectively). If the top of the breast is rolled laterally and the lesion moves laterally, then it can be inferred that it is located in the superior breast. Conversely, if the lesion moves medially on the CC RL view, it can be inferred it is in the inferior breast. Although ultrasound can be performed to locate a one-view finding, it is best to perform the rolled views first to more accurately determine the location to be evaluated sonographically.
Other books
Dying Days by Armand Rosamilia
The Killing Season by Compton, Ralph
Awaken Me Darkly by Gena Showalter
Hell Come Sundown by Nancy A. Collins
Cheating to Survive (Fix It or Get Out) by Christine Ardigo
Highway to Hell by Rosemary Clement-Moore
Daring Dane (Intoxicating Passion #3) by Tatum, Felicia
Tales of a Trail of Life by Ann Graham
Your Goose Is Cooked (A LaTisha Barnhart Mystery) by Moore, S. Dionne