Brain Lock: Free Yourself From Obsessive-Compulsive Behavior (11 page)
Read Brain Lock: Free Yourself From Obsessive-Compulsive Behavior Online
Authors: Jeffrey M. Schwartz,Beverly Beyette

IT’S ALL IN YOUR HEAD
The human brain, which weighs about three pounds and is roughly the size of two fists pressed tightly together, is the most complex and fascinating of all our organs, with its network of about ten billion interconnected nerve cells, or neurons.
Our research on people with OCD at UCLA led us to find that, without question, OCD is a neuropsychiatric illness resulting from a malfunction in the circuitry of the brain. But first, let’s take a look inside a human brain and learn a little more about those parts with their mysterious-sounding names, about their functions, and what goes awry to allow OCD to intrude.
This miniglossary should be helpful. (The key structures are illustrated in Figure 2, opposite.)
•
STRIATUM
: The stratum is composed of two parts, the putamen and the caudate nucleus, which sit next to one another in the core of the brain, deep in the center. The putamen is the automatic transmission for that part of the brain that regulates motor or physical movement, and the caudate nucleus is the automatic transmission and filtering station for the front part of the brain that controls thought.
•
ORBITAL CORTEX
: The orbital cortex is the underside of the front of the brain, the “hot spot” in OCD. The brain’s “error-detection circuit,” it is located directly over the eye sockets. Here, thought and emotion combine. The orbital cortex can inform you that something is right or wrong, whether it is something to approach or avoid.
•
CORTEX
: The cortex is the outer surface of the brain. The frontal cortex is where the most advanced thinking and planning take place.
•
BASAL GANGLIA
: The basal ganglia is essentially the same as the striatum; the terms are almost interchangeable. The caudate
nucleus, which enables us to shift gears from one behavior to another, is part of the basal ganglia.
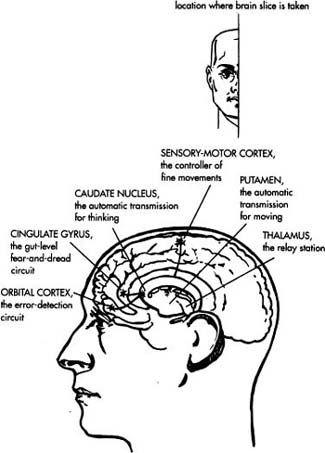
Figure 2. Illustration showing the location of the key structures of the brain that play a part in OCD.
•
CINGULATE GYRUS
: The cingulate gyrus is at the center of the brain, the deepest part of the cortex. It’s wired into your gut and heart-control centers and is responsible for giving you the feeling that something terrible is going to happen if you don’t act on your compulsions to wash, check, whatever.
•
THALAMUS
: The thalamus is the central relay station for processing the body’s sensory information.
The book cover shows color photographs of the brain of Benjamin, a patient at UCLA, before and after cognitive-biobehavioral therapy for the treatment of OCD. (This PET scan image is also shown in Figure 3, on Chapter 2.) Benjamin and other subjects in our UCLA study were injected with a tiny amount of a glucoselike solution that was then trapped in their brains for several hours, enabling us to take pictures and to measure metabolic activity in various parts of the brain. Many people feel relaxed during the scan, perhaps because of the humming of the scanner. Before we inject them, we say, “In the next half hour or so, we’re going to be taking pictures of whatever your brain is doing. If you have obsessions now, that’s what we’re here to record, but whatever happens, happens.” It’s basically at rest, no challenge. Later, when we do the follow-up scan after therapy, we tell them that if obsessions or compulsions arise during the scan, they’re to do the Four Steps, just as they’ve been taught. We have found it extremely helpful to show patients these pictures as a graphic way of helping them understand “It’s not me—it’s my brain.” The knowledge of what’s causing their urges motivates them to work to change from pathological to healthful behavior and, in so doing, to actually change their brain chemistry.
These positron emission tomography (PET) scans clearly demonstrate that the orbital cortex, the underside of the front of the brain, is hypermetabolic, or overheated, in people with OCD (see Figure 1 on Introduction). The colors represent different rates of brain glucose metabolism, or energy use, with red as the hottest and blue as the coolest. One thing these PET scan pictures can tell us is that the more automatic a behavior, the less energy the cortex may require to perform it. For now, keep in mind one key finding: The caudate
nucleus, deep in the core of the brain, which appears to be the source of the primary problem in those with OCD, “cools down” in response to drug therapy, to drug therapy in combination with behavior therapy, and to behavior therapy alone. This is particularly true on the right side of the brain. We can now say we have scientifically demonstrated that by changing your behavior, you can change your brain. If you change your behavioral responses to OCD’s false messages, you will change the brain circuits that cause OCD, which will lead to an improvement in your symptoms.
During the ten years of research that led to this truly ground-breaking finding, my colleagues and I at UCLA undertook a number of experiments that greatly enhanced our understanding of mind-brain interaction.
Dr. John Mazziotta, who heads the Brain Mapping Division of the UCLA Neuropsychiatric Institute, designed an experiment in which the subjects were required to learn to make simple finger-to-thumb rotational movements of the hand, movements that mimicked those used in handwriting. But, because they’d been instructed to make these movements precisely and in a given order, the subjects actually had to think about doing so. What happened—as expected—was that the part of the cortex that controls hand and finger movements became very metabolically activated. In other words, its energy use increased, and it heated up. Next, the subjects were asked to sign their names repeatedly. Now, you know if you’ve ever signed forty traveler’s checks that you don’t think about it a lot after the fourth or fifth check. What we learned was that when the motor task is extremely familiar, the striatum seems to take over. The cortex expends only marginal energy, but the energy use in the striatum increases noticeably. It’s that smooth, automatic transmission in the striatum at work again.
Think of concert pianists: When they first learn to play, they have to think about moving their fingers, which takes considerable energy in the finger-moving part of the cortex. But once they’ve achieved concert-hall status, they move their fingers automatically. Then, they think about the shades and tones of the music. The cortex doesn’t have to expend much energy thinking about moving fingers; the striatum does that. Thus, the advanced parts of the cortex
are freed up to think about the fine points of the music. The experiment with our handwriting subjects gave us insights into this entire process.
When Dr. Mazziotta repeated the signature-signing experiment with a group of subjects with Huntington’s disease, a genetically inherited disease that manifests itself at midlife with the loss of motor control, the results were different. The area of the brain that normally is stimulated by doing an unfamiliar task that requires thinking was stimulated by doing the familiar signature-signing task. Through the degenerative effects of their disease, these subjects’ caudate nucleus and putamen had become mal-functional, and parts of them were dead or dying. The subjects had to use a lot of energy in the cortex to devise strategies to sign their names, since the automatic transmission and filter were broken. They told us it took thought and effort and was hard work. Before the onset of their disease, they could sign their names without giving it a thought. Now, they actually had to control their hands—physically and mentally. They had to use the cortex to take over a function the striatum would normally have been performing. In people with Huntington’s disease, the striatum ultimately disappears, for all intents and purposes, and the abnormal, foreign movements characteristic of their disease, such as writhing and twisting, increase.
Whereas in persons with Huntington’s disease the fact that the automatic transmission and filter are broken causes unwanted movements, in persons with OCD it causes unwanted thoughts and urges, called obsessive thoughts and compulsive urges. Just as the subjects with Huntington’s disease had to apply thought and effort to sign their names because the striatum’s automatic transmission and filtering system were broken, people with OCD have to apply thought and effort when doing behavior therapy to work around the intrusive OCD symptoms. With the automatic screening system of the striatum not working properly, effort must be made to change behaviors while the disturbing thoughts and urges are still there. (You’ll learn more about this process in the next chapter.) But there is one big difference: OCD is largely a fixable problem; at the present time, Huntington’s disease unfortunately is
not, although active research is going on, and there is much hope for progress.
This experiment with people with Huntington’s disease taught us much about the brains of people with OCD. We know that when the striatum is working properly, it acts as a filter, “gating” the sensory information sent to it, which is its proper role in the behavioral loop in the brain. In all likelihood, what happens in OCD is that evolutionary old circuits of the cortex, like those for washing and checking, break through the gate, probably because of a problem in the caudate nucleus. When there is no efficient gating, the person can become overwhelmed by these intrusive urges and act on them in inappropriate ways. These actions are called
behavioral perseverations
, a fancy name for compulsions. Specifically, compulsions are behavioral perseverations that a person knows to be inappropriate and genuinely does not want to be doing: The thought comes in the gate, the gate gets stuck open, and the thought keeps coming in over and over again. People then persevere in washing their hands or checking the stove, even though it makes no sense to do so. These actions may bring them momentary relief, but then—boom—because the gate is stuck open, the urge to wash or check breaks through again and again. To make matters worse, in all probability the more compulsions they do, the more rigidly the gate gets stuck.
In the absence of a fully functioning striatum, the cortex must function in a way that requires conscious effort because unwanted thoughts and urges have a tendency to interfere. It is just this sort of conscious effort that is made in behavior therapy, when a person works to manage responses to intrusive urges.
We have good reason to think that the person with OCD can’t get rid of those intrusive thoughts and urges because the circuit from the orbital cortex, the brain’s “early-warning detection system,” is firing inappropriately. The culprit may well be the lack of proper filtering by the caudate nucleus. Evolution may play a large role in the origins of classic OCD symptoms. Think of the kinds of automatic behaviors that were hardwired into the brain circuitry of our ancestors. In all likelihood, these behaviors had to do with avoiding contamination and checking to make sure that they were safe—that the cave was neither dirty nor dangerous, for example.
STUCK IN GEAR
In behavior therapy, we try to get patients to understand what’s going on in their brains so they can use the cortex to help them stop inappropriate behaviors. Because their automatic transmission is broken, they must use the cortex to shift to another, more appropriate, task. I tell my patients, “You are cursed with a lousy manual transmission. In fact, even your manual doesn’t work great. It’s sticky. It’s hard to shift, but, with effort, you
can
shift those gears yourself.” It’s not easy. It’s hard work because the gearshift is stuck. But when they shift gears repeatedly, by consciously changing behaviors, they actually start to fix their transmission by changing the metabolism of the striatum. Using the cortex, they work around the glitch in the striatum. And the beauty of it is that this technique gets the transmission to slowly start working automatically once again. It becomes easier to shift gears and to change behaviors as you keep working at it. Recent research in the laboratory of my colleague Dr. Lew Baxter may indicate why this is so. He has recently investigated a pathway that sends messages to the basal ganglia from the part of the frontal cortex used for advanced thinking, like the thinking used in applying the Four Steps. This pathway seems to have the ability to help the transmission to shift gears more effectively.
With behavior therapy, there is also a change in the function of the cingulate gyrus, that part of the cortex that is responsible for the feeling that something catastrophic is going to happen if you don’t act on your compulsions. Before treatment, the cingulate gyrus is tightly locked to the orbital cortex, which is probably the reason why obsessive thoughts and urges are accompanied by such terrible feelings of dread. This is one of the major problems in Brain Lock. After the person follows the Four Steps, the orbital cortex and cingulate gyrus uncouple and start to work freely again, and the fear and dread markedly decrease.
Numerous neurological studies have found that when the basal ganglia or striatum is not working properly, automatic motor control is interrupted and the cortex must help out. Conscious thought is required to control shifts from one behavior to another. In a person with Parkinson’s disease, the broken automatic transmission in the
striatum leads to motor rigidity and on-off problems. The gearshift is stuck, and the person must think about each little movement and step.