Better (22 page)
Authors: Atul Gawande

Currently, one baby out of five hundred who are healthy and kicking at thirty-nine weeks dies before or during childbirth--a historically low rate, but obstetricians have reason to believe that scheduled C-sections could avert at least some of these deaths. Many argue that the results for mothers are safe, too. Scheduled C-sections are certainly far less risky than emergency C-sections--procedures done quickly, in dire circumstances, for mothers and babies already in distress. One recent American study has raised concerns about whether scheduled C-sections are safe enough or not, but a study in Britain and one in Israel actually found that scheduled C-sections had lower maternal mortality than vaginal delivery. Mothers who undergo planned C-sections may also (though this remains largely speculation) have fewer problems later in life with incontinence and uterine prolapse.
Yet there is something disquieting about the idea that
childbirth is becoming so readily surgical. Some hospitals across the country are doing Cesarean sections in more than half of child deliveries. It is not merely nostalgic to find this disturbing. We are losing our connection to yet another natural process of life. And we are seeing the waning of the art of childbirth, too. The skill to bring a child in trouble safely through a vaginal delivery, however inconsistent and unevenly distributed, has been nurtured over centuries. In the obstetrical mainstream, it won't be long before it is lost.
Skeptics have noted that Cesarean delivery is suspiciously convenient for obstetrician's schedules and, hour for hour, is paid more handsomely than vaginal birth. Obstetricians say that fear of malpractice suits pushes them to do C-sections more readily than even they consider necessary. Putting so many mothers through surgery is hardly cause for celebration. But our deep-seated desire to limit risk to babies is the biggest force behind its prevalence; it is the price extracted by the reliability we aspire to.
In a sense, there is a tyranny to the score. While we rate the newborn child's health, the mother's pain and blood loss and length of recovery seem to count for little. We have no score for how the mother does, beyond asking whether she lived or not--no measure to prod us to improve results for her, too. Yet this imbalance, at least, can surely be righted. If the child's well-being can be measured, why not the mother's, too? Indeed, we need an Apgar score for everyone who encounters medicine: the psychiatry patient, the patient on the hospital ward, the person going through an operation, and, yes, the mother in childbirth, as well. My research group recently came up with a surgical Apgar score--a ten-point rating
based on the amount of blood loss, the lowest heart rate, and the lowest blood pressure a patient experiences during an operation. Among almost a thousand patients we tested it in, those with a score of nine or ten had a less than 4 percent chance of complications and there were no deaths; those with a score less than five had a greater than 50 percent chance of complications and a 14 percent chance of death. All patients deserve a simple measure that indicates how well or badly they have come through and that pushes the rest of us to innovate. There is no reason we cannot aim for everyone to do better.
"I
WATCHED, YOU
know," Rourke says. "I could see the whole thing in the surgical lights. I saw her head come out!" Katherine Anne was born seven pounds, fifteen ounces, with brown hair, blue-gray eyes, and soft purple welts where her head had been wedged sideways deep inside her mother's pelvis. Her Apgar score was eight at one minute and nine at five minutes--nearly perfect.
Her mother had a harder time. "I was a wreck," Rourke says. "I was so exhausted I was basically stuporous. And I had unbearable pain." She'd gone through almost forty hours of labor and a Cesarean section. Peccei told her the next morning, "You got whipped two ways, and you are going to be a mess." She was so debilitated that her milk did not come in.
"I felt like a complete failure, like everything I had set out to do I failed to do," Rourke says. "I didn't want the epidural and then I begged for the epidural. I didn't want a C-section, and I consented to a C-section. I wanted to breast-feed the
baby, and I utterly failed to breast-feed." She was miserable for a week. "Then one day I realized, 'You know what? This is a stupid thing to think. You have a totally gorgeous little child and it's time to pay a little more attention to your totally gorgeous little child.' Somehow she let me put all my regrets behind me."
*
Earlier in labor, he would have increased the Pitocin dose to far higher amounts than we accept today, in order to bring her cervix to full dilation. Then he would have put the forceps on.
F
inding a meaningful way to measure performance, as Virginia Apgar showed was possible in child delivery, is a form of ingenuity in itself. What you actually do with that measure involves another type of ingenuity, however, and improvement ultimately requires both kinds. One person who has understood this is a Minneapolis doctor who has spent four decades perfecting care for a single, rare, and fatal disease. His experience holds a lesson for all of us. In order to tell you his story, though, I need to first tell you about Annie Page, a young girl who was discovered to have the disease.
Annie Page's illness began with the kinds of small, unexceptional details that mean nothing until seen in hindsight. Like the fact that, when she was a baby, her father sometimes called
her Little Potato Chip, because her skin tasted salty when he kissed her. Or that Annie's mother noticed that her breathing was sometimes a little wheezy, though the pediatrician heard nothing through his stethoscope.
The detail that finally mattered was Annie's size. For a while, Annie's fine-boned petiteness seemed to be just a family trait. Her sister, Lauryn, four years older, had always been at the bottom end of the pediatrician's growth chart for girls her age. By the time Annie was three years old, however, she had fallen off the chart. She stood an acceptable thirty-four inches tall but weighed only twenty-three pounds--less than 98 percent of girls her age. She did not look malnourished, but she didn't look quite healthy, either.
"Failure to thrive" is what it's called, and there can be scores of explanations: pituitary disorders, hypothyroidism, genetic defects in metabolism, inflammatory-bowel disease, lead poisoning, HIV, tapeworm infection. In textbooks, the complete list is at least a page long. Annie's doctor did a thorough workup. Then, at four o'clock on July 27, 1997--"I'll never forget that day," her mother, Honor, says--the pediatrician called the Pages at home with the results of a sweat test.
It's a funny little test. The skin on the inside surface of a child's forearm is cleaned and dried. Two small gauze pads are applied--one soaked with pilocarpine, a medicine that makes skin sweat, and the other with a salt solution. Electrodes are hooked up. Then a mild electric current is turned on for five minutes, driving the pilocarpine into the skin. A reddened, sweaty area about an inch in diameter appears on the skin, and a collection pad of dry filter paper is taped over it to absorb the
sweat for half an hour. A technician then measures the concentration of chloride in the pad.
Over the phone, the doctor told Honor that her daughter's chloride level was far higher than normal. Honor is a hospital pharmacist, and she had come across children with abnormal results like this. "All I knew was that it meant she was going to die," she said quietly when I visited the Pages' home, in the Cincinnati suburb of Loveland. The test showed that Annie had cystic fibrosis.
Cystic fibrosis is a genetic disease. Only a thousand American children per year are diagnosed as having it. Some ten million people in the United States carry the defective gene, but the disorder is recessive: a child will develop the condition only if both parents are carriers and both pass on a copy. The gene--which was discovered, in 1989, sitting out on the long arm of chromosome No. 7--produces a mutant protein that interferes with cells' ability to manage chloride. This is what makes sweat from people with CF so salty. (Salt is sodium chloride, after all.) The chloride defect thickens secretions throughout the body, turning them dry and gluey. In the ducts of the pancreas, the flow of digestive enzymes becomes blocked, making a child less and less able to absorb food. This was the reason Annie had all but stopped growing. The effects on the lungs, however, are what make the disease lethal. Thickened mucus slowly fills the small airways and hardens, shrinking lung capacity. Over time, the disease leaves a child with the equivalent of just one functioning lung. Then half a lung. Then none at all.
The one overwhelming thought in the minds of Honor and Don Page was: We need to get to Children's. Cincinnati Children's Hospital is among the most respected pediatric
hospitals in the country. It was where Albert Sabin invented the oral polio vaccine. The chapter on cystic fibrosis in the
Nelson Textbook of Pediatrics
--the bible of the specialty--was written by one of the hospital's pediatricians. The Pages called and were given an appointment for the next morning.
"We were there for hours, meeting with all the different members of the team," Honor recalled. "They took Annie's blood pressure, measured her oxygen saturation, did some other tests. Then they put us in a room, and the pediatrician sat down with us. He was very kind, but frank, too. He said, 'Do you understand it's a genetic disease? That it's nothing you did, nothing you can catch?' He told us the median survival for patients was thirty years. In Annie's lifetime, he said, we could see that go to forty. For him, he was sharing a great accomplishment in CF care. And the news was better than our worst fears. But only forty! That's not what we wanted to hear."
The team members reviewed the treatments. The Pages were told that they would have to give Annie pancreatic-enzyme pills with the first bite of every meal. They would have to give her supplemental vitamins. They also had to add calories wherever they could--putting tablespoons of butter on everything, giving her ice cream whenever she wanted, and then putting chocolate sauce on it.
A respiratory therapist explained that they would need to do manual chest therapy at least twice a day, half-hour sessions in which they would strike--"percuss"--their daughter's torso with a cupped hand at each of fourteen specific locations on the front, back, and sides in order to loosen the thick secretions and help her to cough them up. They were given prescriptions for inhaled medicines. The doctor told them that Annie would
need to come back once every three months for extended checkups. And then they went home to start their new life. They had been told almost everything they needed to know in order to give Annie her best chance to live as long as possible.
The one thing that the clinicians failed to tell them, however, was that Cincinnati Children's was not, as the Pages supposed, among the country's top centers for children with cystic fibrosis. According to data from that year, it was, at best, an average program. This was no small matter. In 1997, patients at an average center were living to be just over thirty years old; patients at the top center typically lived to be forty-six. By some measures, Cincinnati was well below average. The best predictor of a CF patient's life expectancy is his or her lung function. At Cincinnati, the lung function achieved by patients under the age of twelve--children like Annie--remained in the bottom 25 percent of the country's CF patients. And the doctors there knew it.
I
T USED TO
be assumed that differences among hospitals or doctors in a particular specialty were generally insignificant. If you plotted a graph showing the results of all the centers treating cystic fibrosis--or any other disease, for that matter--people expected that the curve would look something like a shark fin:
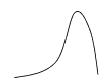
with most places clustered around the very best outcomes. But the evidence has begun to indicate otherwise. What you tend to find instead is a bell curve:
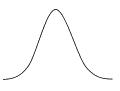
with a handful of teams showing disturbingly poor outcomes for their patients, a handful obtaining remarkably good results, and a great undistinguished middle.