The Coming Plague (119 page)
Authors: Laurie Garrett

9. Microbe Magnets
1
Hippocrates, “On Airs, Waters, and Places,”
The Genuine Works of Hippocrates,
Francis Adams, trans. (London: Leslie P. Adams, Jr., 1849).
The Genuine Works of Hippocrates,
Francis Adams, trans. (London: Leslie P. Adams, Jr., 1849).
2
An ecological description of cities can be found in John Reader,
Man on Earth
(Austin: University of Texas Press, 1988), Chapter 12.
Man on Earth
(Austin: University of Texas Press, 1988), Chapter 12.
3
J. Cairns,
The History of Mortality,
unpublished, 1993.
The History of Mortality,
unpublished, 1993.
4
W. R. MacDonell, “On the Expectation of Life in Ancient Rome, and in the Provinces of Hispania and Lusitania, and Africa,”
Biometrika
9 (1913): 366â80.
Biometrika
9 (1913): 366â80.
5
A. T. Sandison, “Parasitic Diseases,” in D. Brothwell and A. T. Sandison, eds.,
Diseases in Antiquity
(Springfield, IL: Charles C Thomas, 1967).
Diseases in Antiquity
(Springfield, IL: Charles C Thomas, 1967).
6
W. H. McNeill,
Plagues and People
(New York: Doubleday, 1976), Appendix, “Epidemics in China”; and D. Twitchett, “Population and Pestilence in Tâang China,” in W. Baver, ed.,
Studia Sino-Mongolia
(Wiesbaden: Franz Steiner Verlag, 1979), 35â68.
Plagues and People
(New York: Doubleday, 1976), Appendix, “Epidemics in China”; and D. Twitchett, “Population and Pestilence in Tâang China,” in W. Baver, ed.,
Studia Sino-Mongolia
(Wiesbaden: Franz Steiner Verlag, 1979), 35â68.
7
A. Patrick, “Disease in Antiquity: Ancient Greece and Rome,” in Brothwell and Sandison, eds. (1967), op. cit.
8
Jonathan Mann and his colleagues observed cases in the American Southwest during the early 1980s, David Scott studied outbreaks in Ghana in 1908 and 1924, and the World Health Organization reported further outbreaks between 1975 and 1985 in Madagascar, Uganda, Tanzania, Bolivia, Brazil, Peru, Burma, and Vietnam. See World Health Organization. “Human Plague in 1986,”
Weekly Epidemiological Record
62 (1987): 299â300.
Weekly Epidemiological Record
62 (1987): 299â300.
9
Among the most accessible and fascinating accounts of the 1346 Black Death and the later 1665 plague are D. Defoe,
A Journal of the Plague Year
(1722), available in many published forms; McNeill, op. cit., 134â54; B. W. Tuchman,
A Distant Mirror: The Calamitous l4th Century
(New York: Alfred A. Knopf, 1978); and Philip Ziegler,
The Black Death
(London: Collins, 1969).
A Journal of the Plague Year
(1722), available in many published forms; McNeill, op. cit., 134â54; B. W. Tuchman,
A Distant Mirror: The Calamitous l4th Century
(New York: Alfred A. Knopf, 1978); and Philip Ziegler,
The Black Death
(London: Collins, 1969).
10
The trend of blaming the Jews for the Black Death began in what is today called Switzerland and spread quickly throughout Europe. In most cities, the persecutions were started by lower-class tradesmen and peasants who were whipped into frenzies by overzealous monks and priests. In some cities these activities were officially sanctioned by local authorities. In Basel, for example, the town leadership voted to kill all Jews, destroy their homes, and ban Jews from entering the city for another two centuries. On the other hand, there were those in power who opposed such actions and sought to protect Europe's Jewish population. Pope Clement VI gave Jews safe haven inside his papal residence in Avignon. Emperor Charles IV of France tried to stop persecutions in his country, but was overridden by nobles who hoped to avoid paying off debts by letting the mobs kill their Jewish creditors. Duke Albert of Austria was labeled a “Jew-master” because he protected hundreds of Jewish families, allowing them sanctuary inside his fortress. For further details, see J. F. C. Hecker,
The Epidemics of the Middle
Ages, B. G. Babington, trans. (London: Sydenham Society, 1844).
The Epidemics of the Middle
Ages, B. G. Babington, trans. (London: Sydenham Society, 1844).
11
Such a level of microbe-induced mass destruction would not be achieved again until the influenza epidemic of 1918â19. It would be surpassed by AIDS, which over a twenty-year period between 1980 and 2000 is projected to claim an estimated 24 million people, 20 million of whom will have died of the disease by the year 2000. See J. Mann, D. J. M. Tarantola, and T. W. Netter,
AIDS in the World
(Cambridge, MA: Harvard University Press, 1992), 127â32.
AIDS in the World
(Cambridge, MA: Harvard University Press, 1992), 127â32.
12
Earlier circumstantial evidence led Joseph Needham to conclude that China had leprosy prior to A.D. 500, but skeletal studies found no clear leprotic remains in Asia until well after the medieval leprosy epidemic of Europe. See V. Moller-Christensen. “Evidence of Leprosy in Earlier Peoples,” in Brothwell and Sandison, eds. (1967), op. cit. Indeed, the greatest leprosy epidemics of Asia followed European colonialism of the region during the eighteenth century.
13
For these and many other cogent details on the history of tuberculosis, see F. Ryan,
The Forgotten Plague: How the Battle Against Tuberculosis Wa
s
Wonâand Lost
(Boston: Little, Brown, 1993; and R. Dubos, “Tuberculosis,”
Scientific American
181 (1949): 31â40.
The Forgotten Plague: How the Battle Against Tuberculosis Wa
s
Wonâand Lost
(Boston: Little, Brown, 1993; and R. Dubos, “Tuberculosis,”
Scientific American
181 (1949): 31â40.
14
J. B. Bass, Jr., L. S. Farer, P. C. Hopewell, et al., “Diagnostic Standards and Classification of Tuberculosis: Official Statement of the American Thoracic Society,”
American Review of Respiratory Diseases
142 (1990): 725â35.
American Review of Respiratory Diseases
142 (1990): 725â35.
15
R. Riley, “Airborne Infection,”
American Journal of Medicine
57 (1974): 466â75.
American Journal of Medicine
57 (1974): 466â75.
In one particularly ingenious mid-twentieth-century study researchers placed caged guinea pigs in the sealed rooms of human tuberculosis patients. The scientists calculated that, provided the patient's room wasn't aired out, the tiny guinea pig lungs inhaled thirty infectious TB particles a day. The far larger human lung would presumably absorb ten to twenty times as many particles daily under the same circumstances. See R. L. Riley, C. C. Mills, F. O'Grady, et al., “Infectiousness of Air from a Tuberculosis Ward: Ultraviolet Irradiation of Infected Air: Comparative Infectiousness of Different Patients,”
American Review of Respiratory Diseases
84 (1962): 511â25.
American Review of Respiratory Diseases
84 (1962): 511â25.
16
Riley (1974), op. cit.
17
W. L. Salo, A. C. Aufderheide, J. Buikstra, and T. A. Holcomb, “Identification of
Mycobacterium tuberculosis
DNA in a Pre-Columbian Peruvian Mummy,”
Proceedings of the National Academy of Sciences
91 (1994): 2091â94.
Mycobacterium tuberculosis
DNA in a Pre-Columbian Peruvian Mummy,”
Proceedings of the National Academy of Sciences
91 (1994): 2091â94.
18
Consumption was a particular concern. The numbers of cases rose steadily. In Massachusetts, for example, death certificate reports listed consumption (tuberculosis) as the cause of death for 1,634
individuals in 1844; by 1846 that figure was 2,567. And the consumption death reports jumped to 4,593 in 1853. The state's total population in the 1850 census was 994,665. Between 1849 and 1853, a total of 20,000 peopleâmost of them residents of Bostonâdied of consumption. That was about 2 percent of the population. Far more people were sick with the disease, which, like AIDS 120 years later, killed so slowly that statistics never actually reflected at a given moment the full toll of the disease on society.
individuals in 1844; by 1846 that figure was 2,567. And the consumption death reports jumped to 4,593 in 1853. The state's total population in the 1850 census was 994,665. Between 1849 and 1853, a total of 20,000 peopleâmost of them residents of Bostonâdied of consumption. That was about 2 percent of the population. Far more people were sick with the disease, which, like AIDS 120 years later, killed so slowly that statistics never actually reflected at a given moment the full toll of the disease on society.
19
There are several excellent sources for the history of the nineteenth-century cholera pandemics, including D. Barua and W. B. Greenough III,
Current Topics in Infectious Disease: Cholera
(New York: Plenum, 1992); J. Duffy, “Social Impact of Disease in the Late 19th Century,” in J. W. Leavitt and R. L. Numbers, eds.,
Sickness and Health in America
(2nd ed.; Madison: University of Wisconsin, 1985), Chapter 29; and R. J. Evans,
Death in Hamburg: Society and Politics in the Cholera Years 1830â1910
(Oxford, Eng.: Clarendon Press, 1987).
Current Topics in Infectious Disease: Cholera
(New York: Plenum, 1992); J. Duffy, “Social Impact of Disease in the Late 19th Century,” in J. W. Leavitt and R. L. Numbers, eds.,
Sickness and Health in America
(2nd ed.; Madison: University of Wisconsin, 1985), Chapter 29; and R. J. Evans,
Death in Hamburg: Society and Politics in the Cholera Years 1830â1910
(Oxford, Eng.: Clarendon Press, 1987).
20
T. McKeown, R. G. Record, and R. D. Turner, “An Interpretation of the Decline of Mortality in England and Wales During the Twentieth Century,”
Population Studies
29 (1969): 391â422; and T. McKeown and R. G. Record, “Reasons for the Decline of Mortality in England and Wales During the Nineteenth Century,”
Population Studies
16 (1962): 94â122.
Population Studies
29 (1969): 391â422; and T. McKeown and R. G. Record, “Reasons for the Decline of Mortality in England and Wales During the Nineteenth Century,”
Population Studies
16 (1962): 94â122.
21
Select Committee on Population, “Domestic Consequences of United States Population Change,” report prepared for the U.S. House of Representatives, 1978.
22
Noteworthy for the future would be a largely ignored fact in 1970: namely, that tuberculosis skin tests showed that the highest rates of infection in the United States that year were among poor African-American residents of seven Deep South states, and 85 percent of New York City residents who tested positive in TB skin tests that year were blacks who had recently moved to the city from the Deep South.
23
S. O. Freedman, “Tuberculin Testing and Screening: A Critical Evaluation,”
Hospital Practice,
May 1972: 63â70.
Hospital Practice,
May 1972: 63â70.
24
T. McKeown,
The Origins of Haman Disease
(Oxford, Eng.: Basil Blackwell, 1988).
The Origins of Haman Disease
(Oxford, Eng.: Basil Blackwell, 1988).
25
R. Dubos and J. Dubos,
The White Plague: Taberculosis, Man and Society
(Boston: Little, Brown, 1952).
The White Plague: Taberculosis, Man and Society
(Boston: Little, Brown, 1952).
26
B. Bates,
Bargaining for Life: A Social History of Tuberculosis, 1876â1938
(Philadelphia: University of Pennsylvania Press, 1992).
Bargaining for Life: A Social History of Tuberculosis, 1876â1938
(Philadelphia: University of Pennsylvania Press, 1992).
27
B. Bates, “Tuberculosis in Pennsylvania,” in C. E. Rosenberg and J. Golden, eds.,
Framing Disease: Studies in Cultural History
(New Brunswick, NJ: Rutgers University Press, 1992), 229â47.
Framing Disease: Studies in Cultural History
(New Brunswick, NJ: Rutgers University Press, 1992), 229â47.
28
For example, between 1937 and 1947 the numbers of South African families on waiting lists for housing in Johannesburg's black- and colored-designated communities rose from 11 to 16,195. During the subsequent decade the apartheid government decreased its commitment to subsidized housing construction for poor and working-class families from a 1949 high of 7,407 houses to 1957's low of 155. During the same time construction of so-called economic housing, built at government expense for white working- and middle-class families, rose from 348 houses in 1947 to 15,364 in 1957.
29
R. M. Packard,
White Plague, Black Labor: Tuberculosis and the Political Economy of Health and Disease in South Africa
(Berkeley: University of California Press, 1989).
White Plague, Black Labor: Tuberculosis and the Political Economy of Health and Disease in South Africa
(Berkeley: University of California Press, 1989).
30
E. H. Hudson, “Treponematosis and Anthropology,”
Annals of Internal Medicine
58 (1963): 1037.
Annals of Internal Medicine
58 (1963): 1037.
31
Ziegler (1991), op. cit.
32
When the spirochete enters sores on the skin's surface it remains in the vicinity of its initial site of infection. Over time the organism may invade local bone, cartilage, and skin, but infection is rarely systemic. In contrast, sexual transmission of the syphilis spirochete provides immediate access to the blood system, allowing for disease in every organ in the body. The localized yaws infections often resolved without treatment in a matter of weeks, but once syphilis gained entry to the bloodstream most people were fated to suffer systemic illness and, in many cases, slow death.
33
“France: Pitchforked,”
The Economist,
November 28, 1992: 56â57.
The Economist,
November 28, 1992: 56â57.
34
“Pollution in Asia,”
The Economist,
October 6, 1990: 19â21.
The Economist,
October 6, 1990: 19â21.
35
United Nations, “The Prospect of World Urbanization,”
Population Studies
, No. 101, ST/ESA/ SER/101 (New York, 1987).
Population Studies
, No. 101, ST/ESA/ SER/101 (New York, 1987).
36
A. Pryer and N. Crook,
Cities of Hunger: Urban Malnutrition in Developing Countries
(London: Oxfam, 1988).
Cities of Hunger: Urban Malnutrition in Developing Countries
(London: Oxfam, 1988).
37
I. Tabibzadeh, A. Rossi-Espagnet and R. Maxwell,
Spotlight on the Cities: Improving Urban Health in Developing Countries
(Geneva: World Health Organization, 1989).
Spotlight on the Cities: Improving Urban Health in Developing Countries
(Geneva: World Health Organization, 1989).
38
T. Harpham, T. Lusty, and P. Vaughan,
In the Shadow of the City: Community Health and
the Urban Poo
r (Oxford, Eng.: Oxford University Press, 1988); and Tabibzadeh, Rossi-Espagnet, and Maxwell, op. cit.
In the Shadow of the City: Community Health and
the Urban Poo
r (Oxford, Eng.: Oxford University Press, 1988); and Tabibzadeh, Rossi-Espagnet, and Maxwell, op. cit.
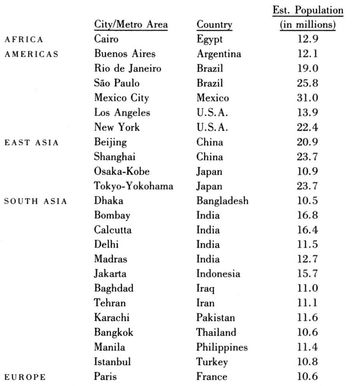
The cities projected to have attained megacity status by 2000 are:
London is expected to drop off the list, as its population is forecast to decline to 9.2 million due to lowering birth rates and middle-class suburban outward migration.
Other books
Patricia Highsmith - The Tremor of Forgery by Patricia Highsmith
The Placebo Effect by David Rotenberg
Body Shrine (Savage Erotica) by Close, Amanda
A Place Within by M.G. Vassanji
Deep by Bates A.L.
Roses and Rodeo (Rough and Ready) by McCray, Cheyenne
The American Sign Language Phrase Book by Fant, Lou, Barbara Bernstein Fant, Betty Miller
Shadow Snatcher by Lou Kuenzler
Besieged by Bertrice Small
Touch Me by Melissa Schroeder