Read Anatomies: A Cultural History of the Human Body Online
Authors: Hugh Aldersey-Williams
Anatomies: A Cultural History of the Human Body (20 page)

I am sent over to one of the couches, where a third nurse inserts the needle in my right (not left!) arm. The scratch is almost completely painless – certainly more skilfully done than when I last had a blood sample taken by the nurse at my GP surgery. Then she starts the machine that over the next ten minutes or so will withdraw 470 millilitres of my blood. I feel a sensation of warmth where the tube carrying the blood is taped to my lower arm – my own departing body heat. Soon the plastic sac is plump with dark red liquid. The quantity is not quite the pint of legend – ‘that’s very nearly an armful’, as the comedian Tony Hancock had it. As I lie there gazing at the roof of the town hall, I ask the nurse what effect she reckons this classic sketch has had on blood donation in Britain. She gives a mirthless laugh and says nothing.
After it is over, I am invited to rest for a few moments and drink more fluids. Regular donors are sitting around comparing notes as to when they first gave blood and what inducements or motivations they had for starting. The local vicar is among them, tucking in to the biscuits. I wonder how much my blood is really worth. Collection is an intensive effort. There are more than a dozen staff at this station. Their target for the session is 115 donors, which will give them something over fifty litres of blood. Is a glass of juice and a three-pack of bourbons fair recompense for my contribution? I ask what happens next to my blood – or the blood that I am still calling mine. I am told it is taken to the National Health Service Blood Transfusion centre in north London to be tested and stored ready for use. Later, I find there is a price put on my blood. The internal market in the NHS means that it is ‘sold’ by NHSBT to hospitals – my 470 millilitres has a price tag of around £125. That’s a lot of biscuits.
I leave the town hall. Does the sunshine seem brighter? The air sharper? I am not sure. Am I light-headed, as I was warned I might be, or is it just the natural adjustment from having been indoors on a glorious spring day? A couple of weeks later, I am impressed when I receive a personal telephone call of thanks. There follows a standard letter confirming my blood group and telling me I have ‘done something truly amazing’. With it comes what I assume is a kind of loyalty card, which I am invited to carry with me. It is red and says I have made ‘1–4 donations’; the highest grade is for those who have made more than 100 donations.
Many academic studies have examined this unusual transaction – a gift system in which donor and recipient are mutually anonymous, in which not all may give, in which no reciprocal gift is exchanged. When asked, donors tend to claim humanitarian motives and altruism as reasons for giving blood, but an underlying selfish satisfaction has also been shown to be a strong factor. I can believe this when I return for my second appointment four months after the first. On this occasion, my blood iron comes in just too low, and I am sent home. The feeling of rejection is surprisingly acute.
Giving blood is a humanitarian act, and one ‘taken in the face of obvious physical costs’, according to one study. It is more obviously a sacrifice than giving money to charity or helping an old lady across the road. Yet giving blood, it is suggested, can become part of oneself, part of what defines a person. The authors draw a comparison with church-going. In one survey asking first-time donors why they chose to give blood, a maintenance fitter is to be found quoting John Donne: ‘No man is an island.’
It is important to know more about donors’ motives in order to promote donation. The standard letter I received from NHS Blood and Transplant tells me that only 5 per cent of people who could donate do so regularly. Repeat donors are worth far more to the health service, although research has focused almost entirely on first-time donors. Money, it seems, is not the answer. Making the exchange a commercial one – giving a fee instead of biscuits – is generally thought to run counter to the high-minded, communitarian motives identified in surveys. It would also be likely to skew the donor profile towards those who need the money, and this in turn would prompt (not always rational) questions about the quality of blood likely to be obtained. In the United States during the 1950s and 1960s, ‘Cash paid for blood’ signs appeared in slum neighbourhoods, and donors were encouraged to give blood in exchange for family credit. Yet the number of donors rose only modestly at this time, while in Britain following the founding of the NHS the rate of donation increased almost fourfold.
Donor enrolment has continued to rise but at a slower pace since, raising the question of how to increase supply in the face of rising demand for blood (although in fact it is also known that the
perception
that there is this ever-present need is a major factor causing first-time donors to come back, and this is exploited by donation agencies). There is talk of finding new ways to increase levels of giving. But there may be limits on what is achievable that go back to our deepest fears about our life-blood. In the 1960s, the notorious American euthanasia activist Jack Kevorkian known as ‘Dr Death’ – and also the author of a musical suite entitled
A Very Still Life
and sometime painter in his own blood – proposed that blood be harvested from fresh human corpses. His early experiments confirmed that cadaveric blood could be used in transfusions, but his work was rejected by hospital colleagues. He suggested in the journal
Military Medicine
in 1964 that the technique might be of use on the battlefield, but failed to interest the Pentagon. The idea might be regarded in principle as no more objectionable than harvesting organs from certificated donors. Blood is just another tissue, after all – one of the connective tissues, so-called because it runs throughout the body rather than being associated exclusively with localized organs. But it seems the cultural barriers are greater than the medical ones.
Perhaps my selfless civic gesture is a relic of the old custom among country people to submit to a bloodletting each spring and autumn equinox. This tradition owes much to Galen, whose thinking shaped both Islamic and Western medicine for many centuries following his death around 200
CE
. Strengthened by medieval attempts to link aspects of human health with the astrological calendar, it became a seasonal ritual which did not entirely die out until well into the nineteenth century. It was usual to let, or drain off, about as much blood as in the sac that I filled for the NHS. I had seen the gory tools used for this in medical museums – the simple lancet, and a scarifying device like a miniature version of a spiked roller for aerating a lawn that could inflict many small, shallow wounds across an area of skin. Bloodletting persisted for centuries, not least because it often worked. It was a practical remedy for people suffering from high blood pressure, heavy menstrual bleeding, haemorrhoids and various inflammations and fevers. It was doubtless also effective as a placebo – as pills are today – as well as having the salutary spiritual effect of inspiring thoughts of Christ on the Cross.
This is not to say there were not occasions where letting blood was absolutely the wrong thing to do. On 14 December 1799, George Washington awoke with a severe cold in the throat. A servant prepared a balm of molasses, vinegar and butter, which the general was unable to swallow. Instead he demanded that half a pint of blood be taken from his arm, having previously used bloodletting to good effect on his slaves. When his physicians arrived, they continued the treatment, the first on the scene draining forty ounces of blood in two venesections, the second taking another thirty-two ounces. It was, as both his servant and his wife Martha had feared, the worst treatment, and by that evening the first president of the United States was dead. He can have had hardly any blood left in his body at the end.
Blood was first among equals of the four humours, the system that governed medical practice for more than two millennia, from before Hippocrates to well after the rise of anatomy and modern medicine with Vesalius and Harvey. The four humours were invisible themselves, but their signs were seen in the blood, phlegm, yellow bile and black bile. Blood carried all the humours through the body as well as the thinner fluid known as the spirit. Phlegm included a range of protein-rich secretions such as tears and sweat as well as nasal mucus. Yellow bile was seen in the pus that appears around a healing wound and in stomach juices. Black bile was seen in congealed blood or an abnormally dark stool. The four humours represented balance in the human microcosm as the four elements (earth, air, fire and water) and the four seasons did in the macrocosm. Illness was regarded as an imbalance in one or more of the humours. Cholerics had an excess of yellow bile associated with the same hot and dry temperaments as the element fire. Phlegmatics were their opposite, cold and damp, like water. Melancholics combined dry and cool, like the earth, while sanguine types were warm and damp, like blood and the air. (It is perhaps an indication of the logical power of this neatly interlocking system that its obvious basis in a Mediterranean climate could be so easily overlooked by physicians in northern Europe, where the air is cold and the earth damp.)
Doctors had no way to supplement a deficiency in any of the humours, so in practice treatment was based on relieving a supposed excess. Bloodletting was the most direct method. An excess of phlegm could be treated with expectorants, yellow bile with emetics, and black bile with laxatives. The whole body became a kind of hydraulic network of channels, overflows and water gates, from which excess fluid must be run off to keep it in good order. The four humours might seem vague and inadequate to us now, but the system that they described was both self-consistent and robust, as its great longevity shows. It was also evidence-based to a remarkable degree. I am left with the conclusion that an equinoctial bloodletting is more likely to do me some good than a modern-day detox, although I think I prefer the rituals of the NHSBT over submission to the scarifier.
The idea of the humours lives on, not only in our continuing belief in the diagnostic value of a blood test, the sound of a cough, the appearance of a stool or of a cut as it heals, but also in our recognition during the past century of the importance of endocrinology. It is now the endocrine system, and the hormones that it releases into our bloodstream, that we understand as governing our metabolism and moods, and we have begun to talk about dopamine and melatonin, endorphins and adrenaline in the same way that the ancients spoke of the unseen humours.
There is a breed of physician whose members I imagine, bow-tied in all probability, stalking the art galleries of the world, searching out artistic depictions of their medical speciality. Usually, they have retired from practice, but they still maintain the fascination with the particular part of the body that brought them into medicine in the first place. So former hepatologists consider the accuracy of Classical scenes showing Prometheus chained to a rock with the eagle pecking at his liver (marvelling perhaps at the nightly regeneration of the organ so that Prometheus must go through it all again the next day). Podiatrists triumphantly spot the artists who, for reasons of compositional elegance or sheer inattention, have given their subjects two left feet. (It happens more often than you might think.)
Inspired by their example, let us consider the strange case of the ear in Dutch art. The ear enjoys a peculiar status in the art of portraiture. It’s generally thought that the hand is the hardest part to draw. Of the facial features, the eyes, nose and mouth are almost unavoidable in any portrait. The ears, though, are somewhat optional. The ears (or more usually, ear) can always be covered by the brim of a hat or an extravagant ruff collar. The ear, it is implied, is an obligato exercise, something that should only be attempted by the most ambitious draughtsman. Even in Vermeer’s
Girl with a Pearl Earring
, only the lobe of the ear from which the famous earring hangs is visible. The gallery-going physicians who have set me off in this particular direction, and to whom I am most grateful, are a plastic surgeon, Wolfgang Pirsig, and a medical historian, Jacques Willemot, who together have edited a volume called
Ear, Nose and Throat in Culture
. They confirm this supposition. ‘It is not surprising to find prominent ears in the works of four outstanding painters who drew most of their portraits with considerable fidelity to nature: Hieronymus Bosch, Leonardo da Vinci, Albrecht Dürer and Rembrandt,’ they write. These artists were notably great draughtsmen as well as great painters.
For most artists, the ears don’t really matter – they are a side issue, quite literally. When I drew the partial dissection of a head, I found the ear unavoidable. I reckoned I had made a fair stab at its outline curve and spent considerable effort on shading the folds, and was pleased with my effort until I noticed that I had located it a good inch too far down on the head. The old masters don’t make such elementary blunders. But they do treat the ear as an unusually malleable and mobile appendage. Indeed, artists often develop a ‘signature ear’ by which work may be identified as theirs – a habit that arises from, but scarcely does justice to, the fact that ear shapes vary more greatly between individuals than many other body features.
The star of Jan van Eyck’s 1436
Madonna with Canon van der Paele
, which hangs in the Groeninge Museum in Bruges, is definitely not the centrally enthroned Madonna or the baby Jesus on her lap. It is the other eponymous subject. The canon is being presented to the Virgin in the setting of the church of St Donatian in Bruges. The Madonna is featureless in appearance and bland in expression, but the canon is full of character and wear. He kneels grumpily on the right of the painting. He has just removed his spectacles (then still a novelty) to reveal a face riven with creases and scars. His set jaw juts through a sea of wobbling jowls. An implacable gaze issues from watery eyes weighed down with heavy bags. He is humbly dressed compared with the Madonna and with St George in armour and St Donatian in brocaded robes and mitre who are attending her. With his plain clothes and crumpled visage, he seems almost as if he has been cut out of a modern photograph and inserted to make a profane collage.
The portrayal was once even more grimly realistic. It seems that Canon van der Paele had a large wart or tumour on his left ear. To his credit, he poses for the artist so that we see his left side. And to
his
credit, the artist painted the wart. In this and other works, it is obvious that van Eyck relished the ugly details of human physiognomy. But today, the wart is not there. Nor is there any explanation of its disappearance. It has been airbrushed from history. According to one account, the wart was overpainted during a restoration of the painting in 1934, but the museum does not respond to my requests for confirmation or denial of this story.
Warts are now known to be the result of viral infection, but up until the seventeenth century they were often associated with witchcraft, so there might have been good reason to omit one from a portrait from the start. Undoubtedly many more warts have been left out of great paintings than have been left in. The retention of such a blemish shows a commitment to truthful realism typically representative of the non-hierarchical ideals of the Northern Renaissance. The most famous wart in art is also by an artist of Netherlandish parentage, Peter Lely, who became highly successful in England, managing the trick of working for both Charles I and, after the Restoration, Charles II, and producing a memorable portrait of Oliver Cromwell in between the two. It is not sure that Cromwell asked to be painted ‘warts and all’, as legend records. Horace Walpole, writing a hundred years after the event, is the source of this quotation. He transcribes an instruction to ‘remark all these roughnesses, pimples, warts and everything as you see me, otherwise I will never pay a farthing for it’. Cromwell did have a prominent wart on his lower lip, as both Lely’s portrait and Cromwell’s death mask attest.
Rembrandt is renowned for the equally unflinching series of self-portraits which he painted throughout his career. In 2003, another of our medics-turned-art critics, Ben Cohen, a retired ear, nose and throat surgeon, noticed that in many of them the artist’s ear appears swollen and damaged. In later portraits, an earring hangs from the undamaged lobe below the hardened tissue of the injured part of the ear. Cohen speculates that Rembrandt was the victim of a botched attempt at ear piercing, but nevertheless went back to get the operation done properly later. ‘He must have been a very determined young man to risk further damage to the ear,’ Cohen writes. As with van Eyck’s depiction of Canon van der Paele’s deformed ear, the picture provides evidence of artistic honesty. Rembrandt could easily have avoided depicting the damaged ear by painting himself from the other side.
Ears acquire a life of their own in
The Garden of Earthly Delights
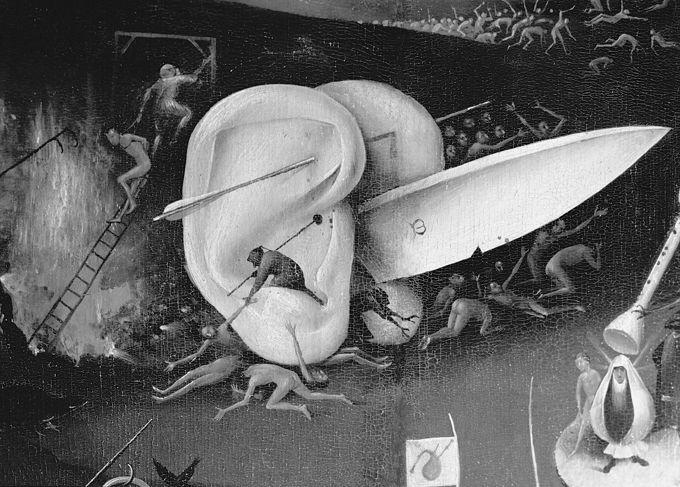
. The triptych by Hieronymus Bosch, painted around the turn of the sixteenth century, is well known, but is so crammed with chaotic goings-on that its details tend to escape proper scrutiny. Its three panels show Adam and Eve in the Garden of Eden on the left, a central scene of paradise crowded with cavorting naked figures, exotic birds and oversize fruit, and a dark scene of hell on the right. This is one of the most fantastical visions in all painting. We see man-eating monsters, acts of bestiality, severed heads and hands and feet, fire and excrement, and even a pig in a nun’s headdress, illustrating a uniquely ingenious set of punishments for the seven deadly sins.
Prominently positioned in the picture, just above the central figure of a man with tree trunks for legs and a broken eggshell for a body who may well be Bosch himself, is a large knife clamped between a giant pair of ears. The arrangement of the ears with the knife thrust forward between them cannot help but suggest male genitals. Lodged within the folds of the ear that faces us is a miniature black figure who appears to be lifting another man in. They may be invading demons, as earrings were originally worn to ward off demons from this orifice, and this ear is unadorned and therefore unguarded. In his free hand, the black figure holds a spear that pierces the flesh of the ear. Both ears are also separately pierced through by a large arrow.
What does this complicated device mean? (Absurdly, you can buy figurines of it, with or without the miniature invaders, from the National Gallery in London, although the painting is actually at the Prado in Madrid.) Bosch’s painting goes far beyond the narrative realism developed by northern European artists in an effort to bring biblical stories home to ordinary parishioners, and creates its own nightmare world worthy of Sigmund Freud. Individual details clearly speak to particular sins. Gluttony and lust are severely punished. We see figures vomiting and one unfortunate with his anus on fire as it passes a succession of black birds. Perhaps the ears are severed in order to cut the flow of gossip and eavesdropping that feeds envy and rage. Who, guilty of such a sin and seeing these perforated ears, would not feel their own ears begin to sting?
Bosch’s hell is also a clamorous place, so full of musical instruments that some of its denizens are stopping their ears against the din. Physicians note that the giant ears, however, lack auditory canals – they cannot hear anyway. The inner and middle ear contain the mechanisms by which we are able to hear, while the outer ear or auricle acts merely as a sound collector, a point brutally made in Quentin Tarantino’s film
Reservoir Dogs
, when the gangster Mr Blonde severs the captive policeman’s ear and then speaks into it to see if its owner can hear him. The auricles capture and direct sound into the inner ear – when people with jug ears request surgery to make them less prominent, they are actually likely to hear a little less well as a result. René Magritte (Belgian, not Dutch) graphically suggests how sound might be funnelled into the ear in a small gouache no less surreal than Bosch’s image. His
Untitled (Shell in the Form of an Ear)
shows a giant vermiform shell lying on a beach; its spiralling recursions are modelled on the human auricle.
The English colloquialism ‘a word in your shell-like’, typically used by somebody about to vouchsafe a confidence, acknowledges this similarity. In fact, your ear is more shell-like than you may realize. Our ability to hear sounds of different pitch relies on the cochlea, a hollow bone shaped like a snail shell in the inner ear. It works a bit like a French horn in reverse. There are tiny hair cells all along this tapering tube, tuned according to where they are positioned, like the strings of a piano. They vibrate in response to different frequencies of sound transmitted into the cochlea by the action of the eardrum on the three tiny bones of the middle ear. These vibrations trigger nerve signals to the brain which we interpret as sound. It is amazing that these thousands of hairs can do their job simultaneously so that, in the Haydn symphony I am listening to as I write, I am able to distinguish each instrument that is playing by its individual pitch and timbre. When we lose the ability to hear high-pitched tones with increasing age, it is because some of these hair cells die off. My mild tone deafness, on the other hand, is not explained by physical shortcomings in the ear but a relative underdevelopment of part of my brain, which could probably be remedied with suitable aural exercises if I ever found the time.
Some people believe the outer ear may be significant other than as a sound-gatherer. In the 1950s, a French doctor and acupuncturist named Paul Nogier noted that it resembles a curled human foetus (the lobe of the ear represents the head and the interior fold known as the antihelix the spine of the foetus in this case). The scheme of alternative medicine that he devised based on this resemblance is known as auriculotherapy. The patient’s ear is seen as a homunculus or map of the whole body, with stimulation at different points on it being used to treat ailments in corresponding parts of the body. The idea is perhaps not dissimilar to the ancient Greek belief that the ear provides a channel, via the mouth and throat, into the core of the body, and has echoes of the cauterization once used as a treatment for gross body pains such as sciatica, in which some of the flesh of the ear might be burned away using a hot iron. Noting that the ear we can see in Bosch’s painting is pierced in two places, Nogier and a colleague took these for acupuncture needle positions and tested the effect on some of their patients. They claim that stimulation at the entry point of their acupuncture needle was effective in suppressing the libido, while stimulation of the exit point heightened sexual interest.
The long hairstyles of the time meant that Antoon van Dyck (who prospered in England during the second quarter of the seventeenth century, going on to be knighted as Sir Anthony) painted many portraits but few ears. One of the exceptions is in an early work, done when the artist was nineteen years old, showing the moment when Christ is captured in the Garden of Gethsemane after his betrayal by Judas. The painting is a chaos of violent action. In the foreground, the apostle Peter is holding Malchus, the servant of the arresting high priest, to the ground and is about to slice off his ear in an effort to prevent the arrest. The ear in question glistens redly as if anticipating the cut. Van Dyck’s Peter wields a short knife rather than the sword mentioned in the Bible, which makes the action seem more like a common street crime close to home. Jesus warns Peter to put away his blade (uttering the familiar ‘all who take the sword will perish by the sword’, in Matthew’s gospel). In the version according to Luke, who was a physician, Jesus also heals the ear by a touch of his hand, the only occasion in the whole of Scripture where he heals a fresh wound. This biblical episode has been a stock subject for artists. Most do not waste the opportunity to show Peter in the bloody act, but a few show the aftermath, either with the ear held triumphantly aloft or with the focus on Jesus’s remedial gesture. Wolfgang Pirsig has counted fifty-four such paintings, with the artists often choosing freely between left and right ears according to compositional convenience, even though two of the gospels specify that it was Malchus’s right ear that was severed. In three careless examples, Christ the healer is actually implanting the wrong ear into the wound on the side of Malchus’s head.
